Qiu Shuo, Zhou Tian, Qiu Bo, Zhang Yuxin, Zhou Yonggang, Yu Huihui, Zhang Jingyi, Liu Li, Yuan Lijun, Yang Guodong, Duan Yunyou, Xing Changyang
Department of Ultrasound Diagnostics, Tangdu Hospital, Air Force Medical University, Xi'an, China.
Department of General Surgery, Tangdu Hospital, Air Force Medical University, Xi'an, China.
Front Cardiovasc Med. 2021 Sep 29;8:736854. doi: 10.3389/fcvm.2021.736854. eCollection 2021.
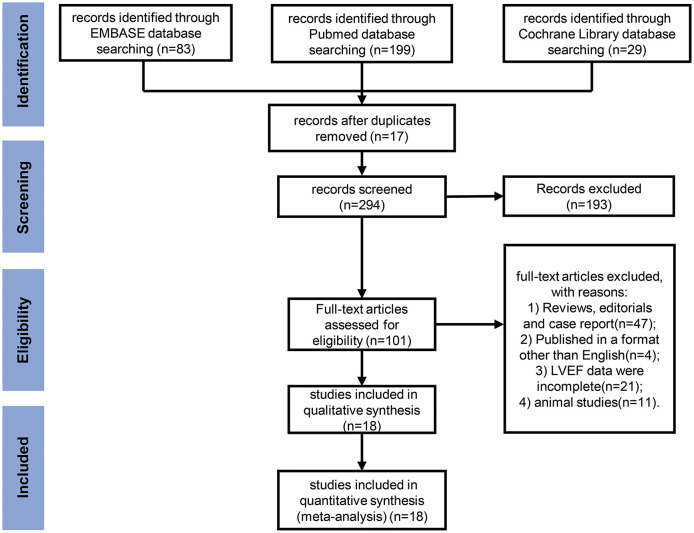
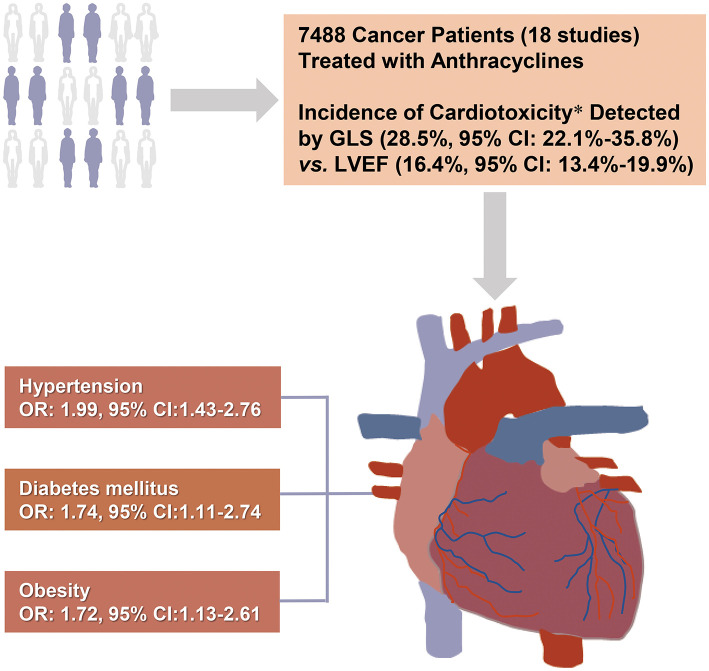
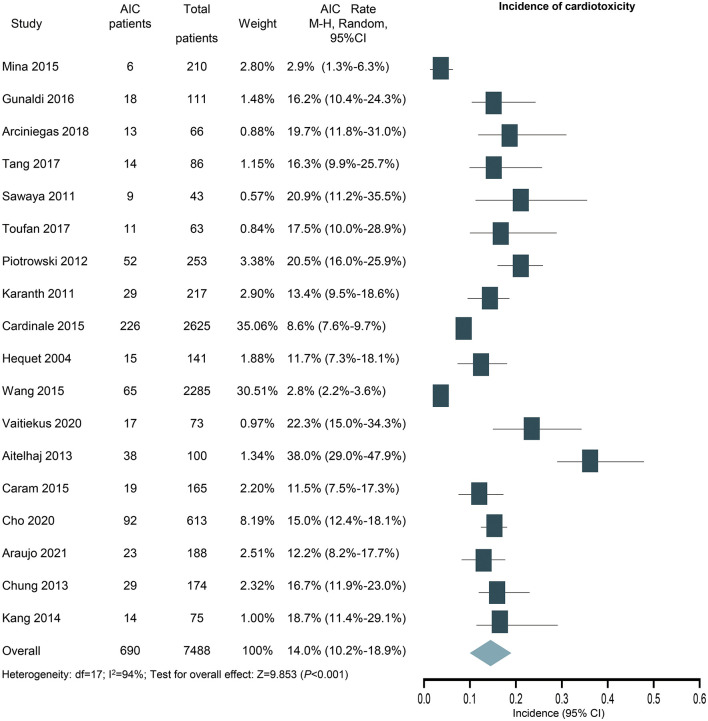
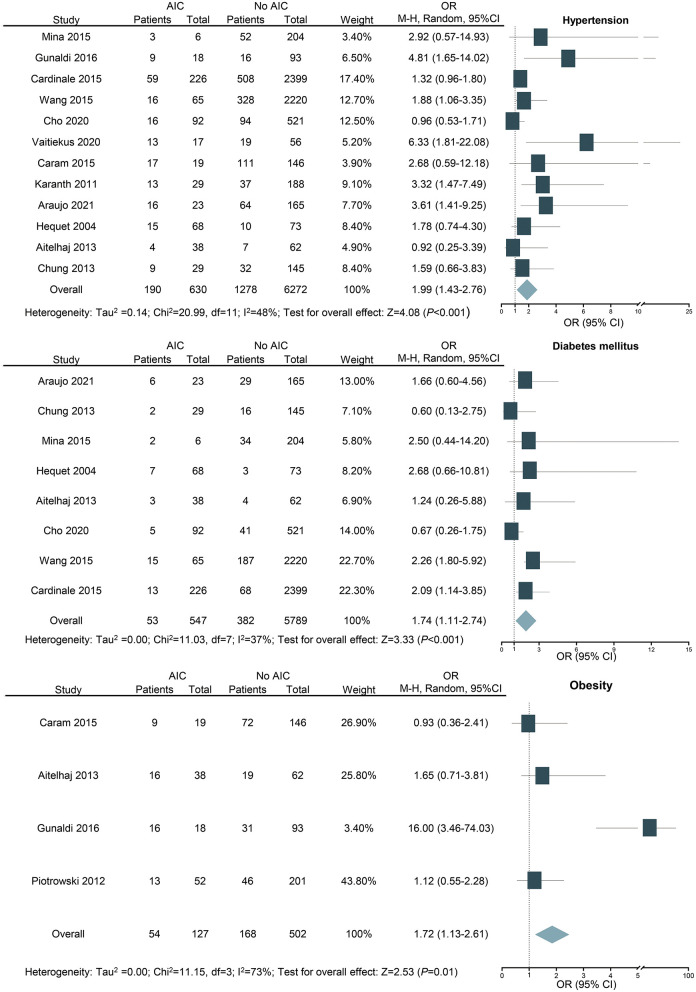
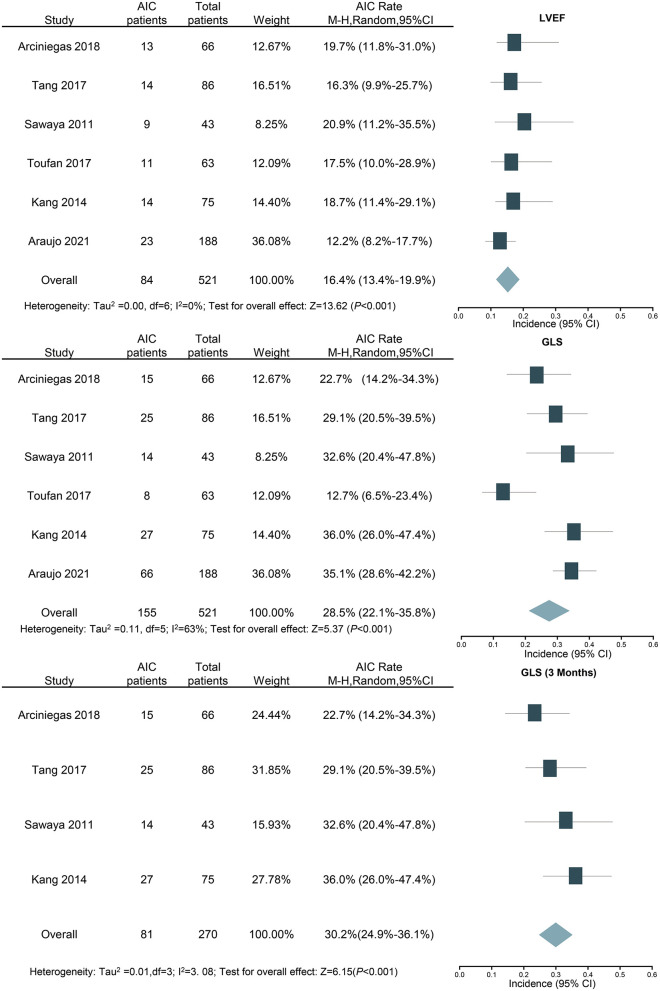
Several cardiovascular risk factors have been suggested to be associated with anthracycline-induced cardiotoxicity, but their quantitative effects have not reached a consensus. We searched PubMed, EMBASE, and Cochrane Library databases for manuscripts published from inception to February 2021, which reported the results of cardiotoxicity due to anthracycline chemotherapy without trastuzumab. Cardiotoxicity defined by any reduction of left ventricular eject fraction (LVEF) to below 50% or a >10% reduction from baseline was defined as the primary endpoint. Odd ratios (OR) with 95% confidence intervals (CI) were calculated using a random-effects model meta-analysis. A total of 7,488 patients receiving anthracycline chemotherapy without trastuzumab were included, who had at least one risk factor at baseline. Hypertension (OR: 1.99; 95% CI: 1.43-2.76), diabetes mellitus (OR: 1.74; 95% CI: 1.11-2.74), and obesity (OR: 1.72; 95% CI: 1.13-2.61) were associated with increased risk of cardiotoxicity. In addition, the relative reduction of global longitudinal strain (GLS) from baseline after anthracycline treatment could significantly improve the detection ability of cardiotoxicity (28.5%, 95% CI: 22.1-35.8% vs. 16.4%, 95% CI: 13.4-19.9%) compared with LVEF. The early detection rate of anthracycline-induced cardiotoxicity (3 months after chemotherapy) by GLS was 30.2% (95% CI: 24.9-36.1%), which is similar with the overall result of GLS. Hypertension, diabetes mellitus, and obesity are associated with increased risk of anthracycline-induced cardiotoxicity, which indicates that corresponding protective strategies should be used during and after anthracycline treatment. The findings of higher detection rate and better early detection ability for cardiotoxicity than LVEF added new proofs for the advantages of GLS in detection of AIC.
已有研究表明,多种心血管危险因素与蒽环类药物所致心脏毒性有关,但其定量影响尚未达成共识。我们检索了PubMed、EMBASE和Cochrane图书馆数据库,查找从数据库建立至2021年2月发表的手稿,这些手稿报告了不含曲妥珠单抗的蒽环类化疗所致心脏毒性的结果。将左心室射血分数(LVEF)降至50%以下或较基线降低超过10%定义的心脏毒性作为主要终点。采用随机效应模型荟萃分析计算比值比(OR)及95%置信区间(CI)。共纳入7488例接受不含曲妥珠单抗的蒽环类化疗且基线时至少有一个危险因素的患者。高血压(OR:1.99;95%CI:1.43 - 2.76)、糖尿病(OR:1.74;95%CI:1.11 - 2.74)和肥胖(OR:1.72;95%CI:1.13 - 2.61)与心脏毒性风险增加相关。此外,与LVEF相比,蒽环类治疗后全球纵向应变(GLS)较基线的相对降低能显著提高心脏毒性的检测能力(28.5%,95%CI:22.1 - 35.8%对16.4%,95%CI:13.4 - 19.9%)。GLS对蒽环类药物所致心脏毒性的早期检测率(化疗后3个月)为30.2%(95%CI:24.9 - 36.1%),与GLS的总体结果相似。高血压、糖尿病和肥胖与蒽环类药物所致心脏毒性风险增加相关,这表明在蒽环类治疗期间及之后应采取相应的保护策略。与LVEF相比,GLS对心脏毒性具有更高的检测率和更好的早期检测能力,这一发现为GLS在检测蒽环类药物所致心脏毒性方面的优势提供了新的证据。