Lodding Isabelle P, Jørgensen Mette, Bennedbæk Marc, Kirkby Nikolai, Naegele Klaudia, Gustafsson Finn, Perch Michael, Rasmussen Allan, Sengeløv Henrik, Sørensen Søren S, Hirsch Hans H, Lundgren Jens D
Centre of Excellence for Health, Immunity and Infections (CHIP), Rigshospitalet, Copenhagen, Denmark.
Department of Haematology, Rigshospitalet, Copenhagen, Denmark.
Open Forum Infect Dis. 2021 Sep 4;8(10):ofab462. doi: 10.1093/ofid/ofab462. eCollection 2021 Oct.
(Val)ganciclovir resistance mutations in CMV UL97 (UL97-GCV-R) complicate anti-CMV therapy in recipients of solid organ and hematopoietic stem cell transplants, but comprehensive data on prevalence, emergence, and outcome are scarce.
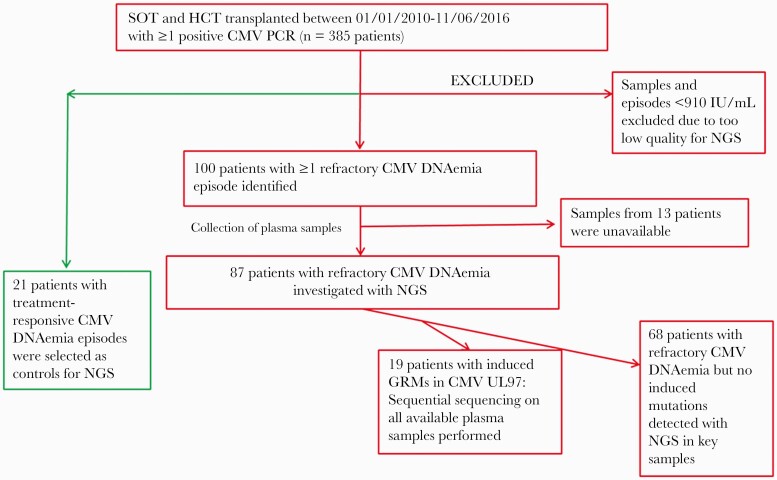
Using next-generation sequencing (NGS; Illumina MiSeq platform), we analyzed UL97-GCV-R in patients with available plasma samples and refractory CMV replication/DNAemia (n = 87) containing viral loads ≥910 IU/mL. Twenty-one patients with CMV DNAemia resolving under antiviral therapy were analyzed as controls. Detected mutations were considered induced and of potential clinical significance if they increased by ≥10% compared with the first detected frequency or if they had a maximum frequency ≥25%.
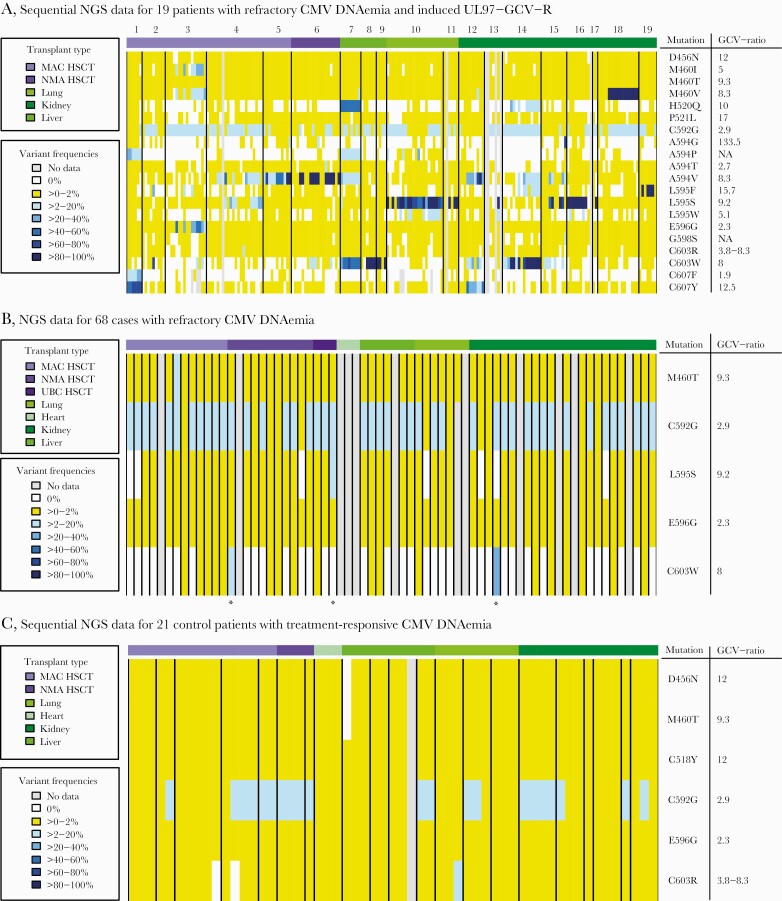
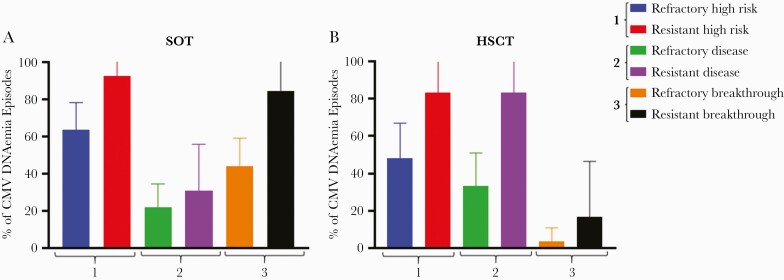
Nineteen of 87 (21.8%) with refractory CMV replication had ≥1 UL97-GCV-R detected by NGS, in comparison to 0/21 of the controls ( = .02). One-third of the recipients had 2 or more induced UL97-GCV-R mutations. The most frequently induced mutations affected codons 595 (42% [8/19]), 594 (32% [6/19]), and 603 (32% [6/19]). C592G was present in all episodes of both cases and controls at frequencies <15%, but never induced. UL97-GCV-R tended to be more frequent in donor/recipient CMV immunoglobulin G mismatch or following failure to complete primary prophylaxis, and many developed invasive CMV disease.
UL97-GCV-R is common among transplant patients with refractory CMV replication. Early testing by NGS allows for identification of major mutations at codons 595, 594, and 603 and excludes a major role of C592G in ganciclovir resistance. Large prospective studies on UL97-GCV-R are warranted.
巨细胞病毒UL97基因(UL97-GCV-R)中的(缬)更昔洛韦耐药突变使实体器官移植和造血干细胞移植受者的抗巨细胞病毒治疗变得复杂,但关于其患病率、出现情况及结果的全面数据稀缺。
我们使用二代测序(NGS;Illumina MiSeq平台)分析了有可用血浆样本且巨细胞病毒复制/病毒血症难治(n = 87)、病毒载量≥910 IU/mL患者的UL97-GCV-R。将21例在抗病毒治疗下巨细胞病毒血症得到缓解的患者作为对照进行分析。如果检测到的突变与首次检测频率相比增加≥10%或其最大频率≥25%,则认为这些突变是诱导产生的且具有潜在临床意义。
87例巨细胞病毒复制难治患者中有19例(21.8%)通过NGS检测到≥1个UL97-GCV-R,而对照组21例中为0例(P = 0.02)。三分之一的受者有2个或更多诱导产生的UL97-GCV-R突变。最常诱导产生的突变影响密码子595(42% [8/19])、594(32% [6/19])和603(32% [6/19])。C592G在病例组和对照组的所有发作中均以<15%的频率存在,但从未被诱导产生。UL97-GCV-R在供体/受者巨细胞病毒免疫球蛋白G不匹配或未完成初级预防后往往更常见,且许多患者发生了侵袭性巨细胞病毒疾病。
UL97-GCV-R在巨细胞病毒复制难治的移植患者中很常见。通过NGS进行早期检测可识别密码子595、594和603处的主要突变,并排除C592G在更昔洛韦耐药中的主要作用。有必要对UL97-GCV-R进行大型前瞻性研究。