Center for the Study of Atherosclerosis, E. Bassini Hospital, Cinisello Balsamo, Milan, Italy.
IRCCS MultiMedica, Sesto S. Giovanni, Milan, Italy.
Curr Atheroscler Rep. 2021 Oct 26;23(12):79. doi: 10.1007/s11883-021-00972-x.
Familial hypercholesterolemia (FH) is a monogenic disorder characterized by high plasma levels of low-density lipoprotein cholesterol (LDL-C) since birth and a high risk of premature cardiovascular disease. The genetic defect is carried in only one allele in heterozygous FH (HeFH) or in both in the most severe homozygous FH (HoFH). Current guidelines recommend to reduce substantially LDL-C levels in these high-risk patients, with the need to use association therapy combining agents with different mechanisms of action. As most cases of FH are attributable to mutations in the gene encoding the low-density lipoprotein receptor (LDLR), statins, even in combination with ezetimibe, are less effective in reducing LDL-C plasma levels in FH patients, who require a more intensive approach with additional lipid-lowering agents. Additional targets playing key roles in regulating LDL-C levels are represented by PCSK9 and ANGPTL3.
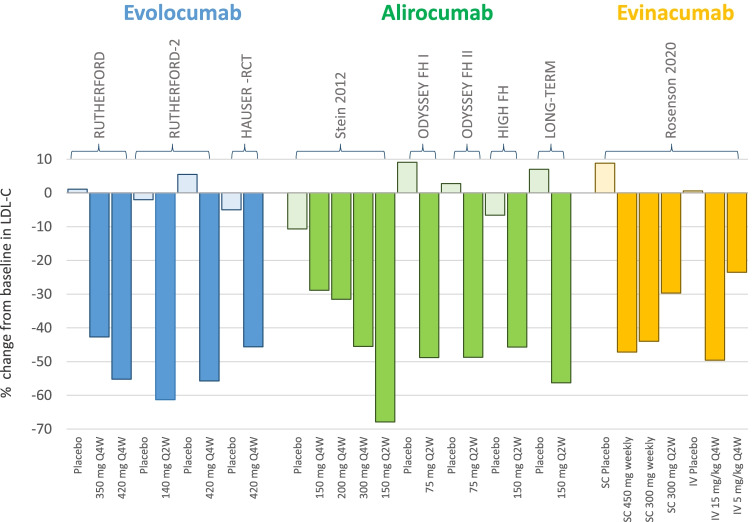
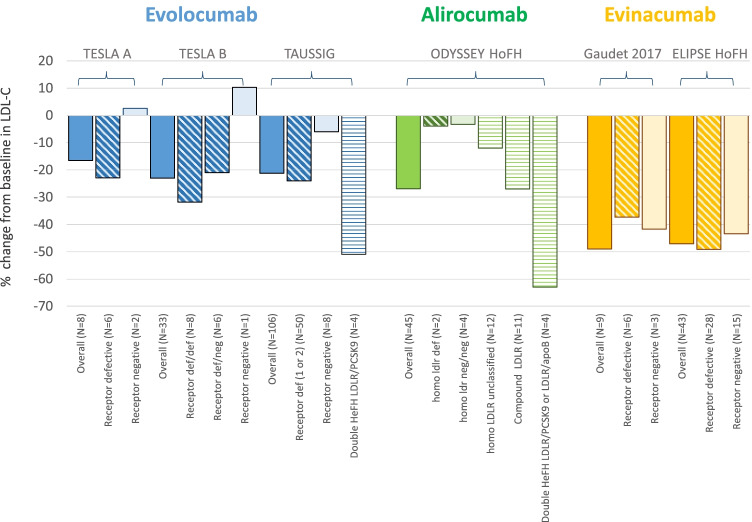
Two monoclonal antibodies (mAbs) targeting PCSK9, evolocumab and alirocumab, significantly reduce LDL-C levels in HeFH patients. In patients with HoFH, the efficacy of mAbs to PCSK9 is strictly related to the presence of a residual LDLR activity; thus, patients carrying null mutations do not respond to the therapy with these mAbs, whereas some effects can be appreciated in HoFH bearing defective mutations. Conversely, evinacumab, the mAb targeting ANGPTL3, is highly effective in reducing LDL-C levels even in HoFH patients carrying null LDLR mutations, thanks to its LDLR-independent mechanism of action. Monoclonal antibodies inhibiting PCSK9 have shown a robust effect in FH patients presenting a residual LDLR activity, while ANGPTL3 inhibitors appear to be promising even in patients carrying null LDLR mutations.
家族性高胆固醇血症(FH)是一种单基因疾病,其特征为自出生起血浆低密度脂蛋白胆固醇(LDL-C)水平升高,且存在早发心血管疾病的高危风险。杂合子 FH(HeFH)中仅一个等位基因携带遗传缺陷,而在最严重的纯合子 FH(HoFH)中则两个等位基因均携带遗传缺陷。目前的指南建议这些高危患者的 LDL-C 水平应大幅降低,需要联合使用具有不同作用机制的药物进行联合治疗。由于大多数 FH 病例归因于编码 LDL 受体(LDLR)的基因突变,因此他汀类药物即使与依折麦布联合使用,对于降低 FH 患者的 LDL-C 血浆水平效果也较差,这些患者需要更强化的治疗方案,联合应用其他降脂药物。在调节 LDL-C 水平方面发挥关键作用的其他靶点包括 PCSK9 和 ANGPTL3。
两种针对 PCSK9 的单克隆抗体(mAb),依洛尤单抗和阿利西尤单抗,可显著降低 HeFH 患者的 LDL-C 水平。在 HoFH 患者中,PCSK9 mAb 的疗效与 LDLR 活性的残留程度密切相关;因此,携带无功能突变的患者对这些 mAb 治疗无反应,而某些突变患者则可观察到一定效果。相反,靶向 ANGPTL3 的 evinacumab 由于其 LDLR 非依赖性作用机制,在携带无功能 LDLR 突变的 HoFH 患者中也能有效降低 LDL-C 水平。抑制 PCSK9 的单克隆抗体在具有残留 LDLR 活性的 FH 患者中表现出强大的疗效,而 ANGPTL3 抑制剂似乎在携带无功能 LDLR 突变的患者中也很有前景。