Anaesthesia, Pain and Critical Care Sciences, School of Physiology, Pharmacology and Neuroscience, University of Bristol, Bristol, UK.
Department of Anaesthesia and Intensive Care Medicine, North Bristol NHS Trust, Bristol, UK.
Anaesthesia. 2022 Jan;77(1):22-27. doi: 10.1111/anae.15599. Epub 2021 Oct 26.
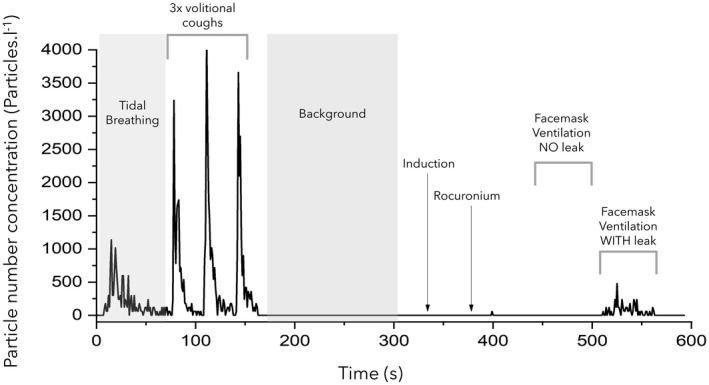
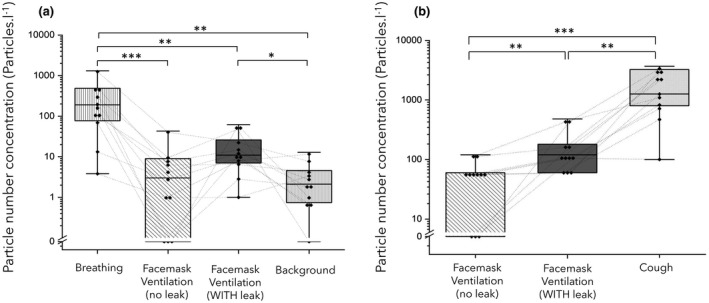
Manual facemask ventilation, a core component of elective and emergency airway management, is classified as an aerosol-generating procedure. This designation is based on one epidemiological study suggesting an association between facemask ventilation and transmission during the SARS-CoV-1 outbreak in 2003. There is no direct evidence to indicate whether facemask ventilation is a high-risk procedure for aerosol generation. We conducted aerosol monitoring during routine facemask ventilation and facemask ventilation with an intentionally generated leak in anaesthetised patients. Recordings were made in ultraclean operating theatres and compared against the aerosol generated by tidal breathing and cough manoeuvres. Respiratory aerosol from tidal breathing in 11 patients was reliably detected above the very low background particle concentrations with median [IQR (range)] particle counts of 191 (77-486 [4-1313]) and 2 (1-5 [0-13]) particles.l , respectively, p = 0.002. The median (IQR [range]) aerosol concentration detected during facemask ventilation without a leak (3 (0-9 [0-43]) particles.l ) and with an intentional leak (11 (7-26 [1-62]) particles.l ) was 64-fold (p = 0.001) and 17-fold (p = 0.002) lower than that of tidal breathing, respectively. Median (IQR [range]) peak particle concentration during facemask ventilation both without a leak (60 (0-60 [0-120]) particles.l ) and with a leak (120 (60-180 [60-480]) particles.l ) were 20-fold (p = 0.002) and 10-fold (0.001) lower than a cough (1260 (800-3242 [100-3682]) particles.l ), respectively. This study demonstrates that facemask ventilation, even when performed with an intentional leak, does not generate high levels of bioaerosol. On the basis of this evidence, we argue facemask ventilation should not be considered an aerosol-generating procedure.
手动面罩通气是择期和紧急气道管理的核心组成部分,被归类为产生气溶胶的程序。这一分类是基于一项流行病学研究,该研究表明面罩通气与 2003 年 SARS-CoV-1 爆发期间的传播之间存在关联。没有直接证据表明面罩通气是否是产生气溶胶的高风险程序。我们在麻醉患者中进行了常规面罩通气和故意产生泄漏的面罩通气期间的气溶胶监测。在超净手术室中进行了记录,并与潮气量呼吸和咳嗽产生的气溶胶进行了比较。在 11 名患者的潮气量呼吸中,呼吸气溶胶可可靠地检测到极低的背景颗粒浓度之上,中位[IQR(范围)]颗粒计数为 191(77-486[4-1313])和 2(1-5[0-13])颗粒/升,p=0.002。在无泄漏面罩通气期间(3[0-9[0-43])颗粒/升)和故意泄漏时(11[7-26[1-62])颗粒/升)检测到的气溶胶浓度中位数(IQR[范围])分别低 64 倍(p=0.001)和 17 倍(p=0.002)。无泄漏面罩通气时(60[0-60[0-120])颗粒/升)和泄漏时(120[60-180[60-480])颗粒/升)的中位(IQR[范围])峰值颗粒浓度分别低 20 倍(p=0.002)和 10 倍(0.001)于咳嗽时(1260[800-3242[100-3682])颗粒/升)。这项研究表明,即使在故意产生泄漏的情况下,面罩通气也不会产生高水平的生物气溶胶。基于这一证据,我们认为面罩通气不应被视为产生气溶胶的程序。