Drakopoulos Fotis, Tsolakis Christos, Angelopoulos Angelos, Liu Yixun, Yao Chengjun, Kavazidi Kyriaki Rafailia, Foroglou Nikolaos, Fedorov Andrey, Frisken Sarah, Kikinis Ron, Golby Alexandra, Chrisochoides Nikos
Center for Real-Time Computing, Old Dominion University, Norfolk, VA, United States.
Department of Computer Science, Old Dominion University, Norfolk, VA, United States.
Front Digit Health. 2021 Feb 18;2:613608. doi: 10.3389/fdgth.2020.613608. eCollection 2020.
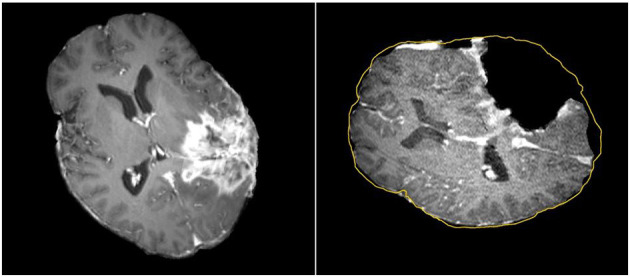
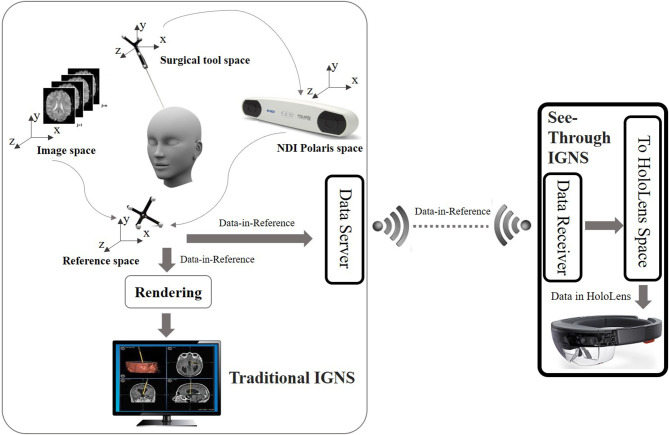
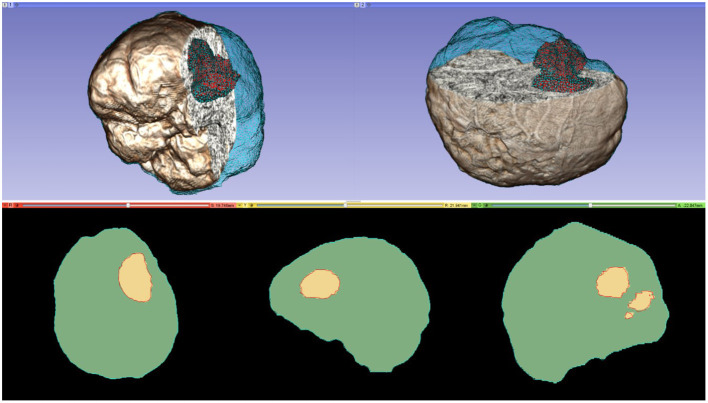
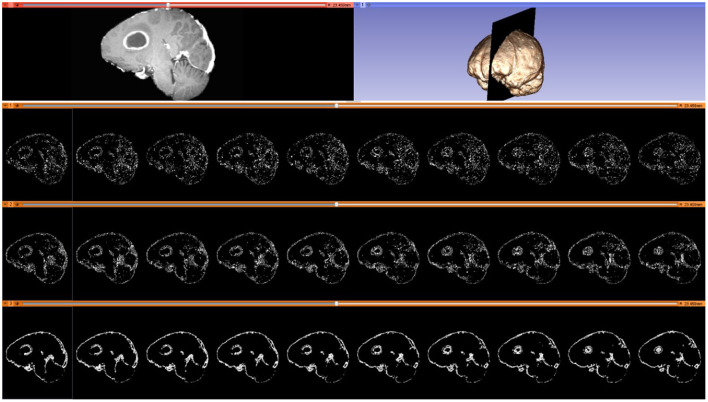
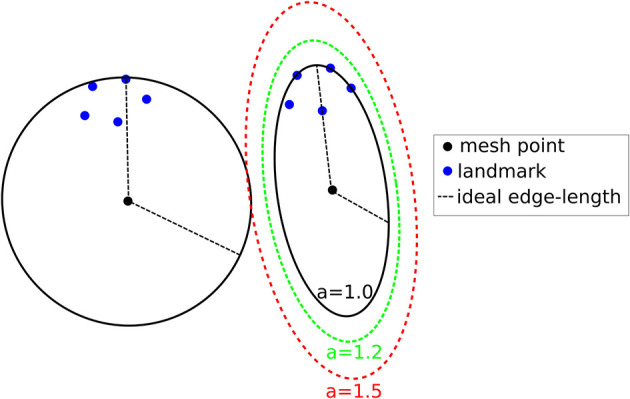
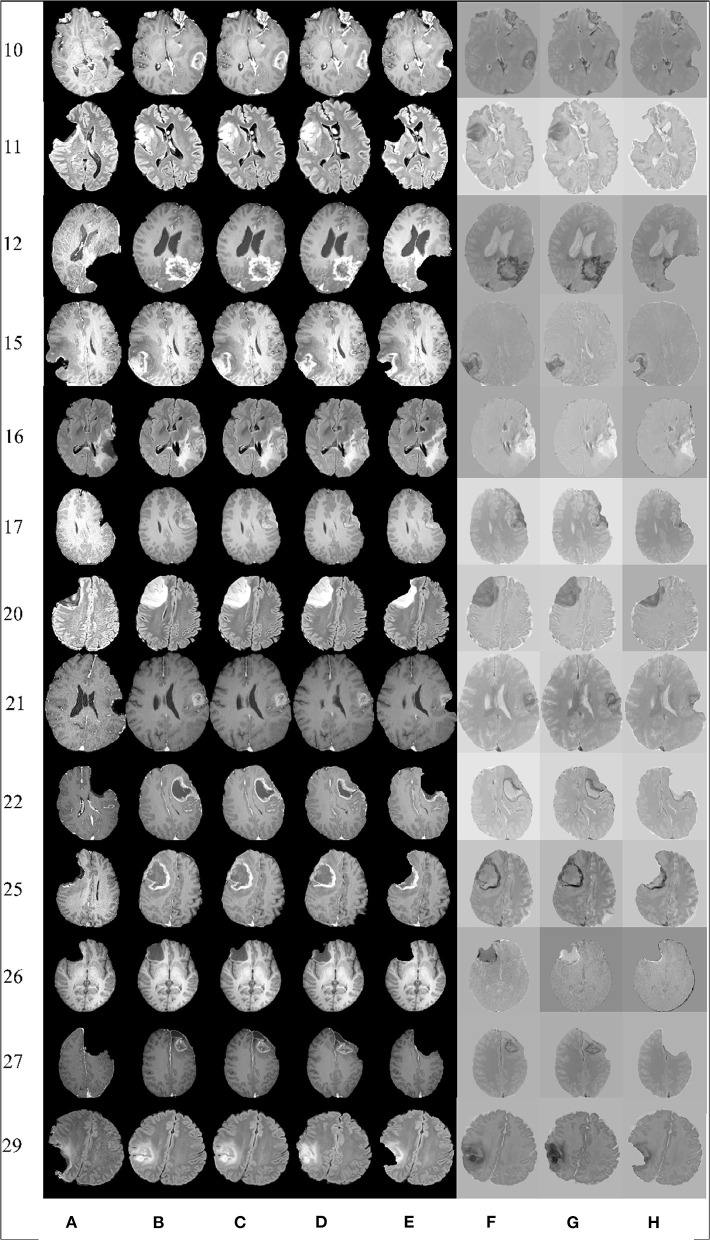
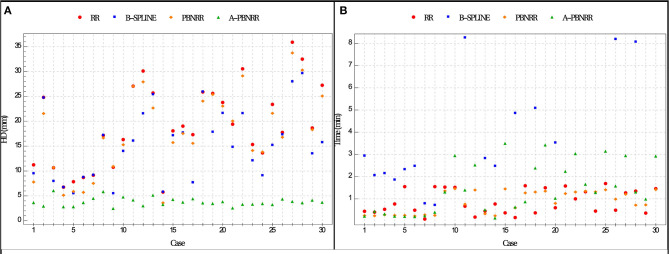
In image-guided neurosurgery, co-registered preoperative anatomical, functional, and diffusion tensor imaging can be used to facilitate a safe resection of brain tumors in eloquent areas of the brain. However, the brain deforms during surgery, particularly in the presence of tumor resection. Non-Rigid Registration (NRR) of the preoperative image data can be used to create a registered image that captures the deformation in the intraoperative image while maintaining the quality of the preoperative image. Using clinical data, this paper reports the results of a comparison of the accuracy and performance among several non-rigid registration methods for handling brain deformation. A new adaptive method that automatically removes mesh elements in the area of the resected tumor, thereby handling deformation in the presence of resection is presented. To improve the user experience, we also present a new way of using mixed reality with ultrasound, MRI, and CT. This study focuses on 30 glioma surgeries performed at two different hospitals, many of which involved the resection of significant tumor volumes. An Adaptive Physics-Based Non-Rigid Registration method (A-PBNRR) registers preoperative and intraoperative MRI for each patient. The results are compared with three other readily available registration methods: a rigid registration implemented in 3D Slicer v4.4.0; a B-Spline non-rigid registration implemented in 3D Slicer v4.4.0; and PBNRR implemented in ITKv4.7.0, upon which A-PBNRR was based. Three measures were employed to facilitate a comprehensive evaluation of the registration accuracy: (i) visual assessment, (ii) a Hausdorff Distance-based metric, and (iii) a landmark-based approach using anatomical points identified by a neurosurgeon. The A-PBNRR using multi-tissue mesh adaptation improved the accuracy of deformable registration by more than five times compared to rigid and traditional physics based non-rigid registration, and four times compared to B-Spline interpolation methods which are part of ITK and 3D Slicer. Performance analysis showed that A-PBNRR could be applied, on average, in <2 min, achieving desirable speed for use in a clinical setting. The A-PBNRR method performed significantly better than other readily available registration methods at modeling deformation in the presence of resection. Both the registration accuracy and performance proved sufficient to be of clinical value in the operating room. A-PBNRR, coupled with the mixed reality system, presents a powerful and affordable solution compared to current neuronavigation systems.
在图像引导的神经外科手术中,术前共配准的解剖、功能和扩散张量成像可用于促进在脑功能区安全切除脑肿瘤。然而,手术过程中大脑会发生变形,尤其是在进行肿瘤切除时。术前图像数据的非刚性配准(NRR)可用于创建一个配准图像,该图像能捕捉术中图像的变形,同时保持术前图像的质量。本文利用临床数据报告了几种处理脑变形的非刚性配准方法在准确性和性能方面的比较结果。提出了一种新的自适应方法,该方法能自动去除切除肿瘤区域的网格元素,从而处理存在切除情况时的变形。为了改善用户体验,我们还提出了一种将混合现实与超声、MRI和CT结合使用的新方法。本研究聚焦于在两家不同医院进行的30例胶质瘤手术,其中许多手术涉及切除较大体积的肿瘤。一种基于自适应物理的非刚性配准方法(A-PBNRR)为每位患者配准术前和术中MRI。将结果与其他三种现成的配准方法进行比较:在3D Slicer v4.4.0中实现的刚性配准;在3D Slicer v4.4.0中实现的B样条非刚性配准;以及在ITKv4.7.0中实现的PBNRR(A-PBNRR基于此)。采用了三种措施来全面评估配准准确性:(i)视觉评估;(ii)基于豪斯多夫距离的度量;(iii)使用神经外科医生确定的解剖点的基于地标方法。与刚性和传统基于物理的非刚性配准相比,使用多组织网格自适应的A-PBNRR将可变形配准的准确性提高了五倍多,与作为ITK和3D Slicer一部分的B样条插值方法相比提高了四倍。性能分析表明,A-PBNRR平均可在不到2分钟内应用,达到了临床环境中使用所需的速度。在模拟存在切除情况时的变形方面,A-PBNRR方法的表现明显优于其他现成的配准方法。配准的准确性和性能都证明足以在手术室中具有临床价值。与当前的神经导航系统相比,A-PBNRR与混合现实系统相结合提供了一种强大且经济实惠的解决方案。