Institute of Clinical Cancer Research (IKF) at Krankenhaus Nordwest, UCT-University Cancer Center, Frankfurt, Germany.
Institut für Klinische Krebsforschung IKF GmbH am Krankenhaus Nordwest, Frankfurt, Germany.
BMC Cancer. 2021 Oct 29;21(1):1158. doi: 10.1186/s12885-021-08872-8.
The main reason for treatment failure after curative surgical resection of gastric cancer is intra-abdominal spread, with 40-50% peritoneal seeding as primary localization of recurrence. Peritoneal relapse is seen in 60-70% of tumors of diffuse type, compared to only 20-30% of intestinal type. Hyperthermic IntraPEritoneal Chemoperfusion (HIPEC) is an increasingly used therapy method for patients with peritoneal metastases. The preventive use of HIPEC could represent an elegant approach for patients (pts) before macroscopic peritoneal seeding, since pts. with operable disease are fit and may have potential risk of microscopic involvement, thus having a theoretical chance of cure with HIPEC even without the need for cytoreduction. No results from a PCRT from the Western hemisphere have yet been published.
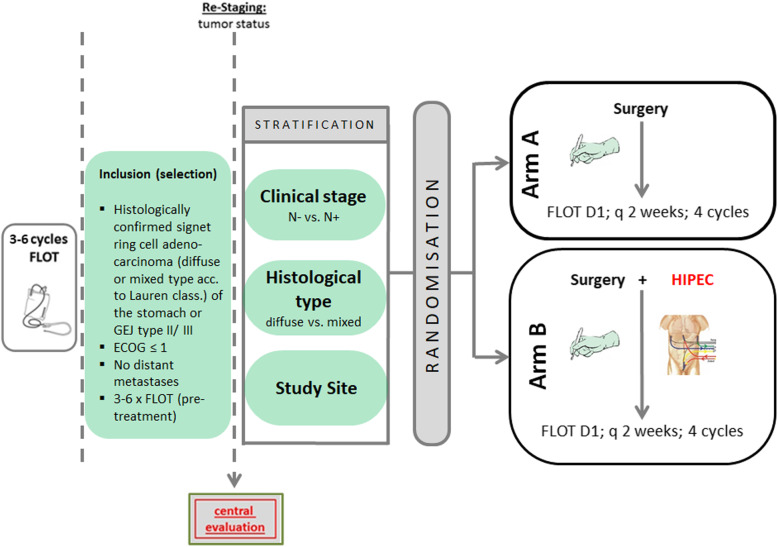
This is a multicenter, randomized, controlled, open-label study including a total of 200 pts. with localized and locally advanced diffuse or mixed type (Laurens's classification) adenocarcinoma of the stomach and Type II/III GEJ. All enrolled pts. will have received 3-6 pre-operative cycles of biweekly FLOT (Docetaxel 50 mg/m; Oxaliplatin 85 mg/m; Leucovorin 200 mg/m; 5-FU 2600 mg/m, q2wk). Pts will be randomized 1:1 to receive surgery only and postoperative FLOT (control arm) or surgery + intraoperative HIPEC (cisplatin 75 mg/m solution administered at a temperature of 42 °C for 90 min) and postoperative FLOT (experimental arm). Surgery is carried out as gastrectomy or transhiatal extended gastrectomy. Primary endpoint is PFS/DFS, major secondary endpoints are OS, rate of pts. with peritoneal relapse at 2 and 3 years, perioperative morbidity/mortality and quality of life. The trial starts with a safety run-in phase. After 20 pts. had curatively intended resection in Arm B, an interim safety analysis is performed. Recruitment has already started and first patient in was on January 18th, 2021.
If the PREVENT concept proves to be effective, this could potentially lead to a new standard of therapy. On the contrary, if the outcome is negative, pts. with gastric cancer and no peritoneal involvement will not be treated with HIPEC during surgery.
The study is registered on June 25th, 2020 under ClinicalTrials.gov Identifier: NCT04447352 ; EudraCT: 2017-003832-35 .
胃癌根治性手术后治疗失败的主要原因是腹腔内播散,40-50%的腹膜种植为复发的主要定位。弥漫型肿瘤中约有 60-70%出现腹膜复发,而肠型肿瘤中只有 20-30%出现腹膜复发。腹腔内热灌注化疗(HIPEC)是一种越来越多地用于治疗腹膜转移患者的治疗方法。预防性使用 HIPEC 可能是一种针对有宏观腹膜种植风险的患者的优雅方法,因为有手术适应证的患者身体状况良好,并且可能有微观浸润的潜在风险,因此即使不需要细胞减灭术,HIPEC 也有理论上的治愈机会。来自西半球的 PCRT 尚无结果公布。
这是一项多中心、随机、对照、开放标签研究,共纳入 200 例局限性和局部晚期弥漫型或混合性(Laurens 分类)胃腺癌和 II/III 型胃食管交界处腺癌患者。所有入组患者均接受 3-6 个周期的每两周一次的 FLOT(多西他赛 50mg/m;奥沙利铂 85mg/m;亚叶酸钙 200mg/m;5-FU 2600mg/m,q2wk)治疗。患者将按照 1:1 的比例随机分为仅接受手术和术后 FLOT(对照组)或手术+术中 HIPEC(顺铂 75mg/m 溶液在 42°C 下给药 90 分钟)和术后 FLOT(实验组)。手术采用胃切除术或经食管裂孔扩大胃切除术进行。主要终点是 PFS/DFS,主要次要终点是 OS、2 年和 3 年时腹膜复发的患者比例、围手术期发病率/死亡率和生活质量。该试验首先进行安全性预试验阶段。在第 B 组中,有 20 例患者进行了根治性切除术,然后进行了中期安全性分析。招募工作已经开始,首位患者于 2021 年 1 月 18 日入组。
如果 PREVENT 概念被证明有效,这可能会成为一种新的治疗标准。相反,如果结果为阴性,没有腹膜受累的胃癌患者在手术期间将不接受 HIPEC 治疗。
该研究于 2020 年 6 月 25 日在 ClinicalTrials.gov 注册,标识符:NCT04447352;EudraCT:2017-003832-35。