Valle Luca F, Bernthal Nicholas, Eilber Fritz C, Shabason Jacob E, Bedi Meena, Kalbasi Anusha
Department of Radiation Oncology, Jonsson Comprehensive Cancer Center and David Geffen School of Medicine, University of California, Los Angeles (UCLA), Los Angeles, CA, USA.
Department of Orthopedic Surgery, Jonsson Comprehensive Cancer Center and David Geffen School of Medicine, University of California, Los Angeles (UCLA), Los Angeles, CA, USA.
Sarcoma. 2021 Oct 26;2021:3735874. doi: 10.1155/2021/3735874. eCollection 2021.
Data supporting hypofractionated preoperative radiation therapy (RT) for patients with extremity and trunk soft tissue sarcoma (STS) are currently limited to phase II single-institution studies. We sought to understand the type and thresholds of clinical evidence required for experts to adopt hypofractionated RT as a standard-of-care option for patients with STS.
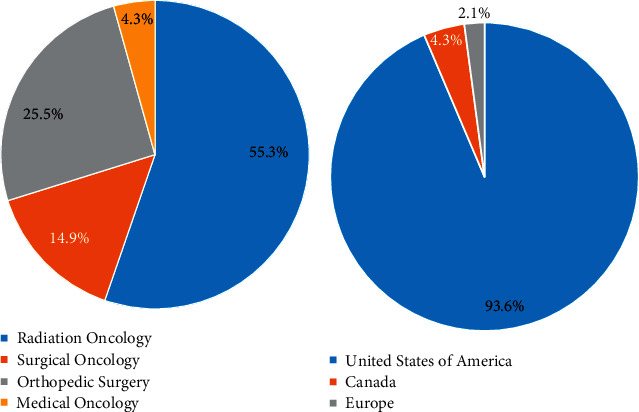
An electronic survey was distributed to multidisciplinary sarcoma experts. The survey queried whether data from a theoretical, multi-institutional, phase II study of 5-fraction preoperative RT could change practice. Using endpoints from RTOG 0630 as a reference, the survey also queried thresholds for acceptable local control, wound complication, and late toxicity for the study protocol to be accepted as a standard-of-care option. Responses were logged from 8/27/2020 to 9/8/2020 and summarized graphically.
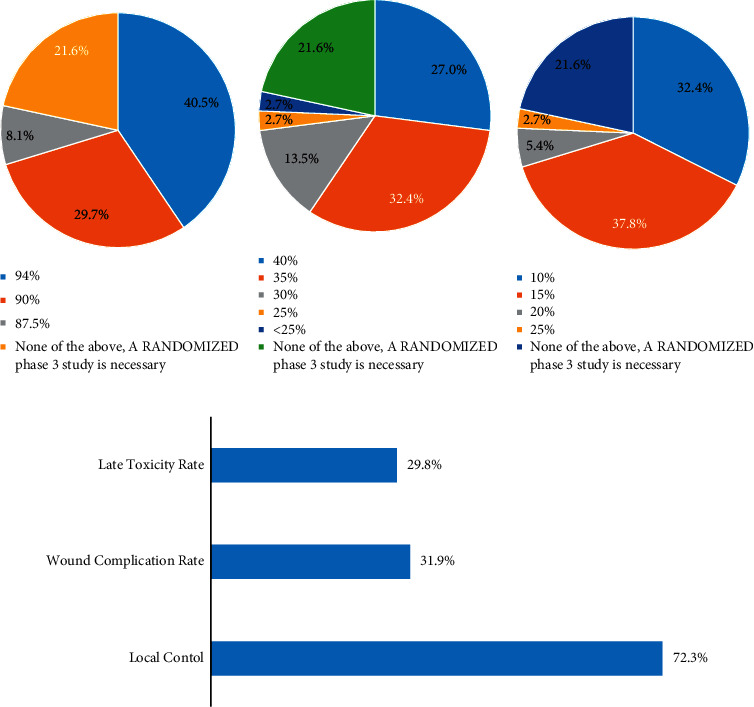
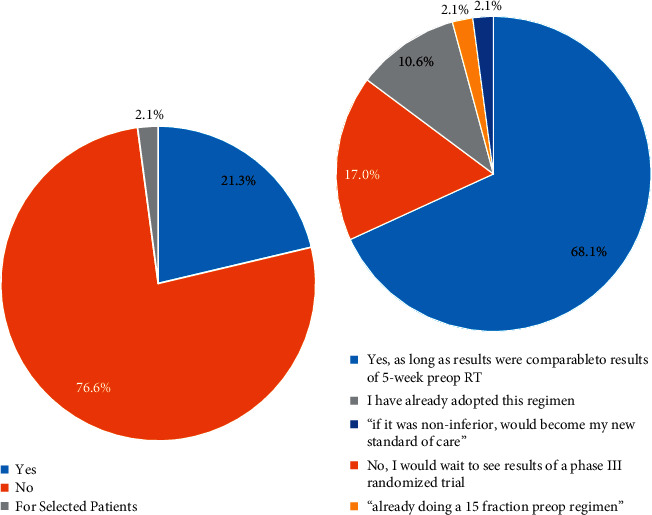
The survey response rate was 55.3% (47/85). Local control is the most important clinical outcome for sarcoma specialists when evaluating whether an RT regimen should be considered standard of care. 17% (8/47) of providers require randomized phase III evidence to consider hypofractionated preoperative RT as a standard-of-care option, whereas 10.6% (5/47) of providers already view this as a standard-of-care option. Of providers willing to change practice based on phase II data, most (78%, 29/37) would accept local control rates equivalent to or less than those in RTOG 0630, as long as the rate was higher than 85%. However, 51.3% (19/37) would require wound complication rates superior to those reported in RTOG 0630, and 46% (17/37) of respondents would accept late toxicity rates inferior to RTOG 0630.
Consensus building is needed among clinicians regarding the type and threshold of evidence needed to evaluate hypofractionated RT as a standard-of-care option. A collaborative consortium-based approach may be the most pragmatic means for developing consensus protocols and pooling data to gradually introduce hypofractionated preoperative RT into routine practice.
目前,支持对肢体和躯干软组织肉瘤(STS)患者进行大分割术前放射治疗(RT)的数据仅限于II期单机构研究。我们试图了解专家将大分割RT作为STS患者护理标准选项所需的临床证据类型和阈值。
向多学科肉瘤专家发放了一份电子调查问卷。该调查询问了一项理论上的多机构II期5分割术前RT研究的数据是否会改变实践。以RTOG 0630的终点为参考,该调查还询问了研究方案被接受为护理标准选项时可接受的局部控制、伤口并发症和晚期毒性的阈值。从2020年8月27日至2020年9月8日记录了回复,并以图形方式进行了总结。
调查回复率为55.3%(47/85)。在评估RT方案是否应被视为护理标准时,局部控制是肉瘤专家最重要的临床结果。17%(8/47)的提供者需要随机III期证据才能将大分割术前RT视为护理标准选项,而10.6%(5/47)的提供者已经将其视为护理标准选项。在愿意根据II期数据改变实践的提供者中,大多数(78%,29/37)只要局部控制率高于85%,就会接受等于或低于RTOG 0630中的局部控制率。然而,51.3%(19/37)的人要求伤口并发症率优于RTOG 0630中报告的率,46%(17/37)的受访者会接受低于RTOG 0630的晚期毒性率。
临床医生之间需要就评估大分割RT作为护理标准选项所需的证据类型和阈值达成共识。基于合作联盟的方法可能是制定共识方案和汇总数据以逐步将大分割术前RT引入常规实践的最务实手段。