Department of Women's Health, Guy's and St Thomas' NHS Foundation Trust, London, UK
Department of Women and Children's Health, King's College London, London, UK.
BMJ Open. 2021 Nov 1;11(11):e049991. doi: 10.1136/bmjopen-2021-049991.
(1) To report maternal and newborn outcomes of pregnant women in areas of social deprivation in inner city London. (2) To compare the effect of caseload midwifery with standard care on maternal and newborn outcomes in this cohort of women.
Retrospective observational cohort study.
Four council wards (electoral districts) in inner city London, where over 90% of residents are in the two most deprived quintiles of the English Index of Multiple Deprivation (IMD) (2019) and the population is ethnically diverse.
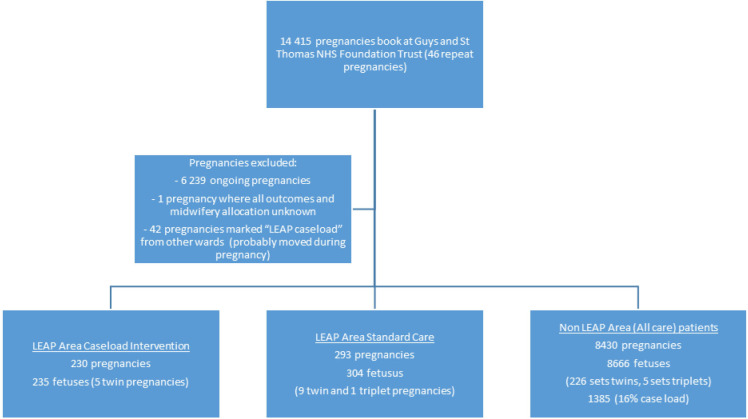
All women booked for antenatal care under Guys and St Thomas' National Health Service Foundation Trust after 11 July 2018 (when the Lambeth Early Action Partnership (LEAP*) caseload midwifery team was implemented) until data collection 18 June 2020. This included 523 pregnancies in the LEAP area, of which 230 were allocated to caseload midwifery, and 8430 pregnancies from other areas.
To explore if targeted caseload midwifery (known to reduce preterm birth) will improve important measurable outcomes (preterm birth, mode of birth and newborn outcomes).
There was a significant reduction in preterm birth rate in women allocated to caseload midwifery, when compared with those who received traditional midwifery care (5.1% vs 11.2%; risk ratio: 0.41; p=0.02; 95% CI 0.18 to 0.86; number needed to treat: 11.9). Caesarean section births were significantly reduced in women allocated to caseload midwifery care, when compared with traditional midwifery care (24.3% vs 38.0%; risk ratio: 0.64: p=0.01; 95% CI 0.47 to 0.90; number needed to treat: 7.4) including emergency caesarean deliveries (15.2% vs 22.5%; risk ratio: 0.59; p=0.03; 95% CI 0.38 to 0.94; number needed to treat: 10) without increase in neonatal unit admission or stillbirth.
This study shows that a model of caseload midwifery care implemented in an inner city deprived community improves outcome by significantly reducing preterm birth and birth by caesarean section when compared with traditional care. This data trend suggests that when applied to targeted groups (women in higher IMD quintile and women of diverse ethnicity) that the impact of intervention is greater.
(1)报告伦敦内城贫困地区孕妇的母婴结局。(2)比较产妇人数助产与标准护理对该队列妇女母婴结局的影响。
回顾性观察队列研究。
伦敦内城的四个议会选区(选区),那里超过 90%的居民处于英国多重剥夺指数(IMD)的两个最贫困五分位数(2019 年),人口种族多样。
2018 年 7 月 11 日后在盖兹和圣托马斯国民保健信托基金接受产前护理预约的所有妇女(当时实施了兰贝斯早期行动伙伴关系(LEAP*)产妇人数助产团队),直至 2020 年 6 月 18 日数据收集。这包括 LEAP 地区的 523 例妊娠,其中 230 例分配给产妇人数助产,以及其他地区的 8430 例妊娠。
探讨有针对性的产妇人数助产(已知可降低早产率)是否会改善重要的可衡量结局(早产、分娩方式和新生儿结局)。
与接受传统助产护理的妇女相比,分配给产妇人数助产的妇女早产率显著降低(5.1% vs 11.2%;风险比:0.41;p=0.02;95%CI 0.18 至 0.86;需要治疗的人数:11.9)。与传统助产护理相比,分配给产妇人数助产的妇女剖宫产分娩显著减少(24.3% vs 38.0%;风险比:0.64:p=0.01;95%CI 0.47 至 0.90;需要治疗的人数:7.4),包括紧急剖宫产分娩(15.2% vs 22.5%;风险比:0.59;p=0.03;95%CI 0.38 至 0.94;需要治疗的人数:10),而新生儿重症监护病房入院率或死产率没有增加。
这项研究表明,在贫困社区实施的产妇人数助产模式通过显著降低早产率和剖宫产率来改善结局,与传统护理相比。这一数据趋势表明,当应用于目标群体(IMD 五分位数较高的妇女和种族多样的妇女)时,干预的效果更大。