Department of Internal Medicine V, Heidelberg University Hospital, Heidelberg, Germany.
Institute of Medical Biometry and Informatics, University of Heidelberg, Heidelberg, Germany.
Trials. 2021 Nov 3;22(1):765. doi: 10.1186/s13063-021-05703-w.
Overall survival remains poor in older patients with acute myeloid leukemia (AML) with less than 10% being alive after 5 years. In recent studies, a significant improvement in event-free, relapse-free and overall survival was shown by adding gemtuzumab ozogamicin (GO), a humanized antibody-drug conjugate directed against CD33, to intensive induction therapy once or in a sequential dosing schedule. Glasdegib, the small-molecule inhibitor of smoothened (SMO), also showed improved overall survival in patients not eligible for intensive chemotherapy when combined with low-dose cytarabine compared to low-dose cytarabine alone. These findings warrant further investigations in the phase III GnG trial.
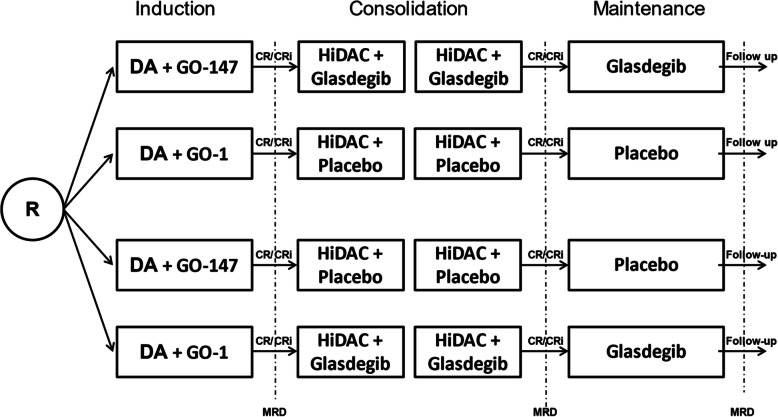
METHODS/DESIGN: This is a randomized phase III trial with measurable residual disease (MRD) after induction therapy and event-free survival (EFS) as primary endpoints. The two research questions are addressed in a 2 by 2 factorial design. Patients age 60 years and older are upfront randomized 1:1 in one of the two induction arms: GO administered to intensive induction therapy on days 1,4, and 7 versus GO administered once on day 1 (GO-147 versus GO-1), and double-blinded 1:1 in one of the subsequent treatment arms glasdegib vs. placebo as adjunct to consolidation therapy and as single-agent maintenance therapy for six months. Chemotherapy backbone for induction therapy consists of standard 7 + 3 schedule with cytarabine 200 mg/m continuously days 1 to 7, daunorubicin 60 mg/m days 1, 2, and 3 and high-dose cytarabine (1 g/m, bi-daily, days 1, 2, and 3) for consolidation therapy. Addressing two primary endpoints, MRD-negativity after induction therapy and event-free survival (EFS), 252 evaluable patients are needed to reject each of the two null hypotheses at a two-sided significance level of 2.5% with a power of at least 85%.
Ethical approval and approvals from the local and federal competent authorities were granted. Trial results will be reported via peer-reviewed journals and presented at conferences and scientific meetings.
Protocol version: 1st version 20.10.2020, no amendments yet. Study initiation on February 16, 2021. First patient was recruited on April 1st.
ClinicalTrials.gov NCT04093505 ; EudraCT 2019-003913-32. Registered on October 30, 2018.
年龄较大的急性髓系白血病(AML)患者的总生存率仍然很差,不到 10%的患者在 5 年后仍然存活。在最近的研究中,通过在强化诱导治疗中添加吉妥珠单抗奥佐米星(GO),一种针对 CD33 的人源化抗体药物偶联物,与单次或序贯给药方案相比,无事件生存、无复发生存和总生存得到了显著改善。小分子 smoothened(SMO)抑制剂glasdegib 与低剂量阿糖胞苷联合使用时,在不符合强化化疗条件的患者中也提高了总生存率。这些发现证明 GnG 试验的 III 期研究是合理的。
方法/设计:这是一项具有可测量残留疾病(MRD)的随机 III 期试验,诱导治疗后无事件生存(EFS)是主要终点。这两个研究问题采用 2×2 析因设计进行探讨。年龄在 60 岁及以上的患者在两个诱导臂之一中进行前瞻性 1:1 随机分组:GO 于诱导治疗第 1、4 和 7 天给予强化诱导治疗与 GO 于第 1 天给予单次给药(GO-147 与 GO-1),随后以双盲 1:1 在后续治疗臂之一中glasdegib 与安慰剂进行随机分组,作为巩固治疗的辅助治疗和 6 个月的单药维持治疗。诱导治疗的化疗方案包括标准的 7+3 方案,阿糖胞苷 200mg/m2 持续输注第 1 至 7 天,柔红霉素 60mg/m2 第 1、2 和 3 天,高剂量阿糖胞苷(1g/m2,每日 2 次,第 1、2 和 3 天)用于巩固治疗。为了检验两个主要终点,即诱导治疗后 MRD 阴性和无事件生存(EFS),需要 252 名可评估患者来拒绝每个双侧显著性水平为 2.5%、至少 85%功效的两个零假设。
已获得伦理批准和当地及联邦主管部门的批准。试验结果将通过同行评议的期刊报告,并在会议和科学会议上展示。
方案版本:2020 年 10 月第 1 版,尚未修订。于 2021 年 2 月 16 日开始研究。首位患者于 4 月 1 日入组。
ClinicalTrials.gov NCT04093505;EudraCT 2019-003913-32。于 2018 年 10 月 30 日注册。