Cowell John K, Hu Tianxiang
Georgia Cancer Center, 1410 Laney Walker Blvd, Augusta, GA 30912, USA.
Cancer Drug Resist. 2021;4(3):607-619. doi: 10.20517/cdr.2021.30. Epub 2021 May 25.
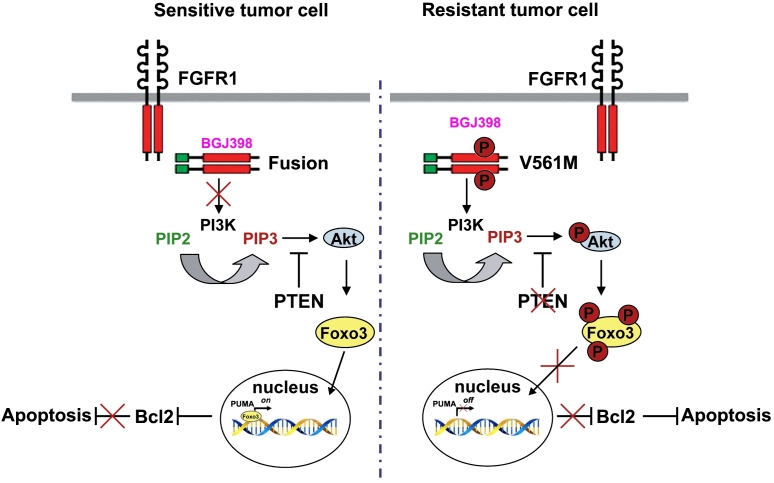
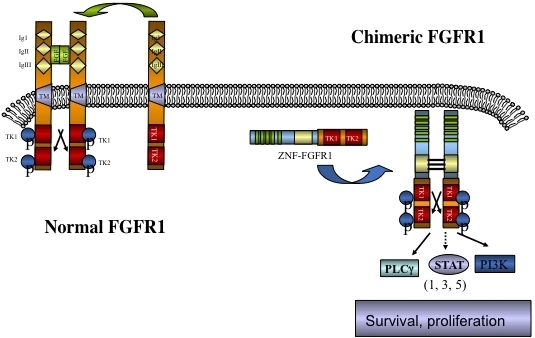
Myeloid and lymphoid neoplasms with eosinophilia and FGFR1 rearrangements (MLN-eo FGFR1) disease is derived from a pluripotent hematopoietic stem cell and has a complex presentation with a myeloproliferative disorder with or without eosinophilia and frequently presents with mixed lineage T- or B-lymphomas. The myeloproliferative disease frequently progresses to AML and lymphoid neoplasms can develop into acute lymphomas. No matter the cell type involved, or clinical presentation, chromosome translocations involving the kinase and various partner genes, which leads to constitutive activation of downstream oncogenic signaling cascades. These patients are not responsive to treatment regimens developed for other acute leukemias and survival is poor. Recent development of specific FGFR1 inhibitors has suggested an alternative therapeutic approach but resistance is likely to evolve over time. Mouse models of this disease syndrome have been developed and are being used for preclinical evaluation of FGFR1 inhibitors. Cell lines from these models have now been developed and have been used to investigate the mechanisms of resistance that might be expected in clinical cases. So far, a mutation in the kinases domain and deletion of have been recognized as leading to resistance and both operate through the PI3K/AKT signaling axis. One of the important consequences is the suppression of PUMA, a potent enforcer of apoptosis, which operates through BCL2. Targeting BCL2 in the resistant cells leads to suppression of leukemia development in mouse models, which potentially provides an opportunity to treat patients that become resistant to FGFR1 inhibitors. In addition, elucidation of molecular mechanisms underlying FGFR1-driven leukemias and lymphomas also provides new targets for combined treatment as another option to bypass the FGFR1 inhibitor resistance and improve patient outcome.
伴有嗜酸性粒细胞增多和FGFR1重排的髓系和淋系肿瘤(MLN-eo FGFR1)疾病源自多能造血干细胞,临床表现复杂,伴有或不伴有嗜酸性粒细胞增多的骨髓增殖性疾病,且常伴有混合谱系T或B淋巴瘤。骨髓增殖性疾病常进展为急性髓系白血病,淋系肿瘤可发展为急性淋巴瘤。无论涉及何种细胞类型或临床表现,涉及该激酶和各种伙伴基因的染色体易位都会导致下游致癌信号级联的组成性激活。这些患者对为其他急性白血病制定的治疗方案无反应,生存率低。最近特异性FGFR1抑制剂的开发提出了一种替代治疗方法,但随着时间的推移可能会产生耐药性。已经建立了这种疾病综合征的小鼠模型,并用于FGFR1抑制剂的临床前评估。现在已经从这些模型中开发出细胞系,并用于研究临床病例中可能出现的耐药机制。到目前为止,该激酶结构域中的一个突变和 的缺失已被认为是导致耐药的原因,两者均通过PI3K/AKT信号轴发挥作用。一个重要的后果是抑制PUMA,PUMA是一种通过BCL2发挥作用的强大凋亡执行者。在耐药细胞中靶向BCL2可导致小鼠模型中白血病发展的抑制,这可能为治疗对FGFR1抑制剂产生耐药性的患者提供机会。此外,阐明FGFR1驱动的白血病和淋巴瘤的分子机制也为联合治疗提供了新的靶点,作为绕过FGFR1抑制剂耐药性并改善患者预后的另一种选择。