Department of Anaesthesia, Intensive Care and Peri-operative Medicine, Hôpital Tenon, Paris, France.
Department of Anaesthesiology, KU Leuven and University Hospital Leuven, Leuven, Belgium.
Anaesthesia. 2022 Mar;77(3):311-325. doi: 10.1111/anae.15609. Epub 2021 Nov 5.
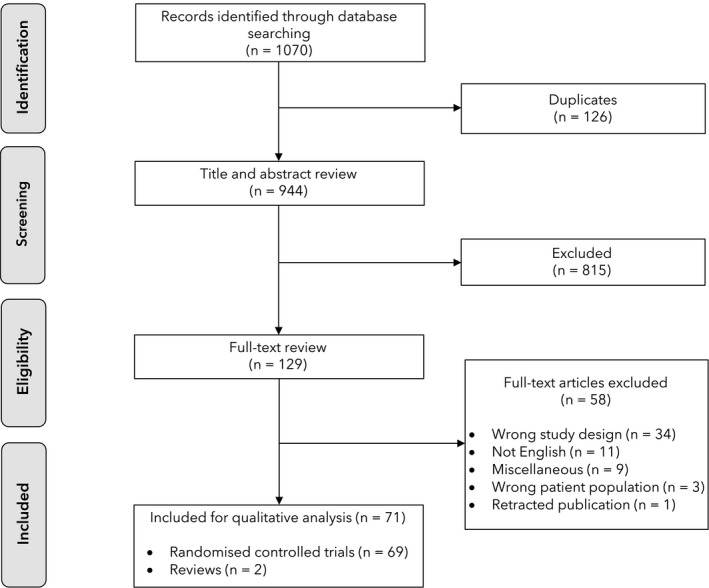
Video-assisted thoracoscopic surgery has become increasingly popular due to faster recovery times and reduced postoperative pain compared with thoracotomy. However, analgesic regimens for video-assisted thoracoscopic surgery vary significantly. The goal of this systematic review was to evaluate the available literature and develop recommendations for optimal pain management after video-assisted thoracoscopic surgery. A systematic review was undertaken using procedure-specific postoperative pain management (PROSPECT) methodology. Randomised controlled trials published in the English language, between January 2010 and January 2021 assessing the effect of analgesic, anaesthetic or surgical interventions were identified. We retrieved 1070 studies of which 69 randomised controlled trials and two reviews met inclusion criteria. We recommend the administration of basic analgesia including paracetamol and non-steroidal anti-inflammatory drugs or cyclo-oxygenase-2-specific inhibitors pre-operatively or intra-operatively and continued postoperatively. Intra-operative intravenous dexmedetomidine infusion may be used, specifically when basic analgesia and regional analgesic techniques could not be given. In addition, a paravertebral block or erector spinae plane block is recommended as a first-choice option. A serratus anterior plane block could also be administered as a second-choice option. Opioids should be reserved as rescue analgesics in the postoperative period.
由于与开胸手术相比,视频辅助胸腔镜手术具有更快的恢复时间和更少的术后疼痛,因此越来越受欢迎。然而,视频辅助胸腔镜手术的镇痛方案差异很大。本系统评价的目的是评估现有文献并为视频辅助胸腔镜手术后的最佳疼痛管理制定建议。使用特定于手术的术后疼痛管理(PROSPECT)方法进行系统评价。检索了 2010 年 1 月至 2021 年 1 月期间发表的评估镇痛、麻醉或手术干预效果的英文随机对照试验。我们检索到 1070 项研究,其中 69 项随机对照试验和 2 项综述符合纳入标准。我们建议在术前或术中给予基本的镇痛药物,包括对乙酰氨基酚和非甾体抗炎药或环氧化酶-2 特异性抑制剂,并在术后继续使用。当不能给予基本镇痛和区域镇痛技术时,可考虑术中静脉给予右美托咪定。此外,椎旁阻滞或竖脊肌平面阻滞是首选方案。也可以作为二线选择给予前锯肌平面阻滞。在术后期间,应将阿片类药物保留为解救性镇痛药。