Ma Wenrui, Pan Qinyuan, Pan Defeng, Xu Tongda, Zhu Hong, Li Dongye
Institute of Cardiovascular Disease Research, Xuzhou Medical University, Xuzhou, China.
Xuzhou Medical University Affiliated Hospital, Xuzhou, China.
Front Pharmacol. 2021 Oct 21;12:713007. doi: 10.3389/fphar.2021.713007. eCollection 2021.
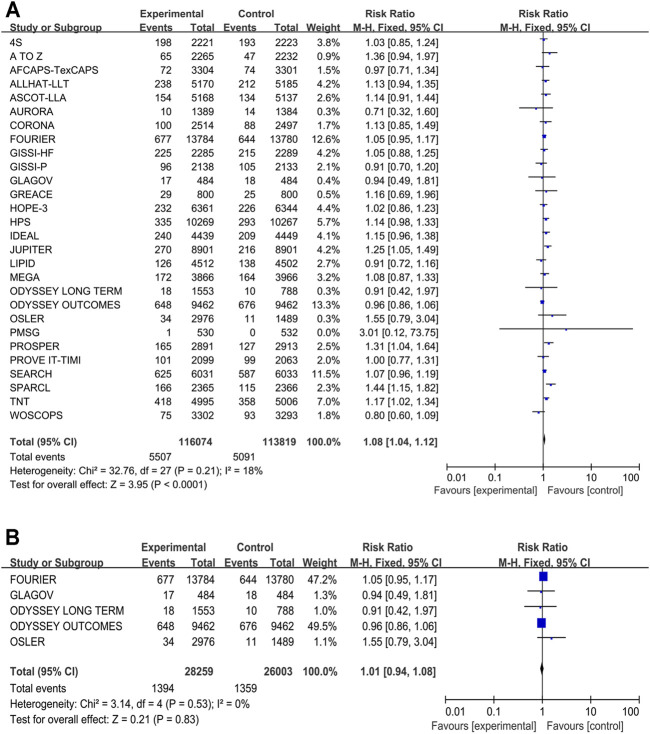
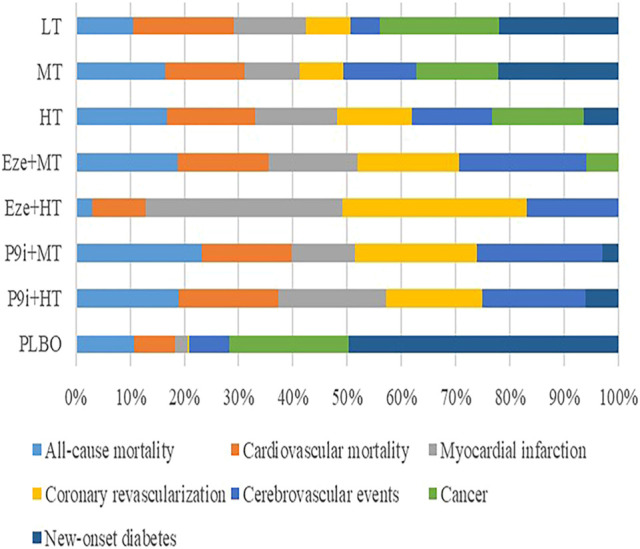
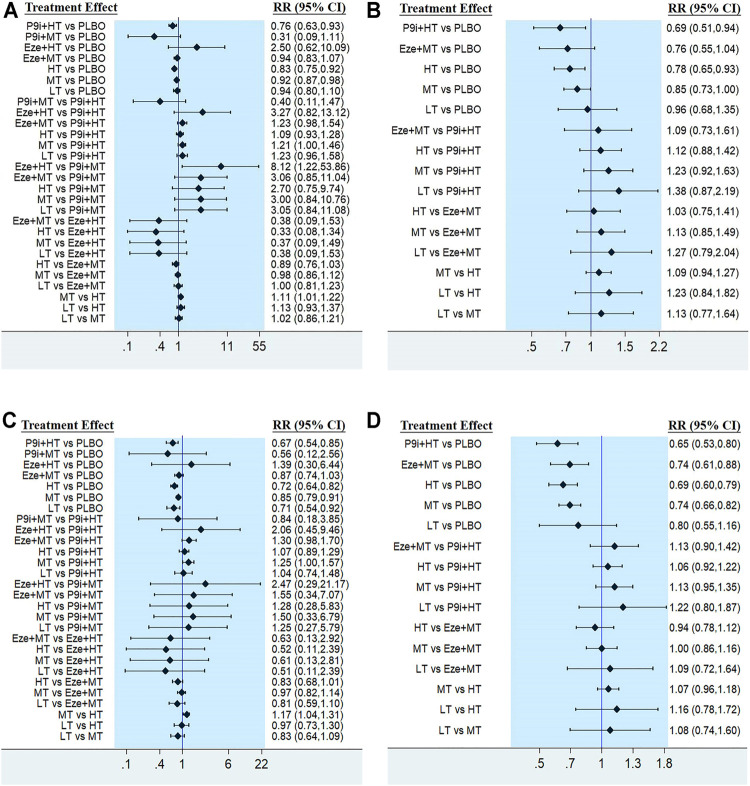
There have been many meta-analyses for statins, ezetimibe and proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9i) to evaluate clinical outcomes, but the efficacy and safety of different intensity of these three drugs on clinical outcomes was absent. PCSK9i, ezetimibe, and statins were divided into seven interventions as follows: including PCSK9i + high-intensity statins (P9i+HT), PCSK9i + moderate-intensity statins (P9i+MT), ezetimibe + high-intensity statins (Eze+HT), ezetimibe + moderate-intensity statins (Eze+MT), high-intensity statins (HT), moderate-intensity statins (MT), and low-intensity statins (LT). The risk ratios (RR) and 95% confidence intervals (CI) were calculated to evaluate the clinical outcomes in all randomized controlled trials included. In traditional meta-analysis, the more intensive treatment had a lower risk of all-cause mortality (RR 0.91, 95% CI 0.88-0.95), cardiovascular mortality (RR 0.89, 95% CI 0.86-0.92), myocardial infarction (RR 0.79, 95% CI 0.77-0.81), coronary revascularization (RR 0.80, 95% CI 0.76-0.84), and cerebrovascular events (RR 0.84, 95% CI 0.80-0.88) compared with the less intensive treatment. However, the more intensive treatment had a higher risk of new-onset diabetes (RR 1.08, 95% CI 1.04-1.12). The network meta-analysis demonstrated that P9i+HT, P9i+MT, HT, and MT were significantly associated with a risk reduction in coronary revascularization and cerebrovascular events compared with PLBO. LT could effectively reduce the risk of cardiovascular mortality (RR 0.71, 95% CI 0.54-0.92), MI (RR 0.67, 95% CI 0.54-0.82), and coronary revascularization (RR 0.77, 95% CI 0.65-0.91) compared with PLBO. P9i+HT was superior to HT in reducing the risk of MI (RR 0.78, 95% CI 0.68-0.90), coronary revascularization (RR 0.84, 95% CI 0.73-0.96), and cerebrovascular events (RR 0.78, 95% CI 0.64-0.95). However, compared with PLBO, P9i+HT, HT, and MT could increase the risk of new-onset diabetes (RR 1.23, 95% CI 1.11-1.37; RR 1.23, 95% CI 1.14-1.33; RR 1.09, 95% CI 1.02-1.15, respectively). In conclusion, PCSK9i added to background statins may be recommended as preferred lipid-lowering therapy, and did not increase the additional risk of new-onset diabetes. The safety and efficacy of ezetimibe was not superior to that of statins. LT can be recommended as the initial therapy.
已有许多关于他汀类药物、依折麦布和前蛋白转化酶枯草溶菌素9型抑制剂(PCSK9i)的荟萃分析来评估临床结局,但这三种药物不同强度对临床结局的疗效和安全性尚缺乏研究。PCSK9i、依折麦布和他汀类药物被分为以下七种干预措施:包括PCSK9i+高强度他汀类药物(P9i+HT)、PCSK9i+中等强度他汀类药物(P9i+MT)、依折麦布+高强度他汀类药物(Eze+HT)、依折麦布+中等强度他汀类药物(Eze+MT)、高强度他汀类药物(HT)、中等强度他汀类药物(MT)和低强度他汀类药物(LT)。计算风险比(RR)和95%置信区间(CI)以评估纳入的所有随机对照试验中的临床结局。在传统荟萃分析中,与强度较低的治疗相比,强度较高的治疗在全因死亡率(RR 0.91,95%CI 0.88-0.95)、心血管死亡率(RR 0.89,95%CI 0.86-0.92)、心肌梗死(RR 0.79,95%CI 0.77-0.81)、冠状动脉血运重建(RR 0.80,95%CI 0.76-0.84)和脑血管事件(RR 0.84,95%CI 0.80-0.88)方面具有较低风险。然而,强度较高的治疗新发糖尿病风险较高(RR 1.08,95%CI 1.04-1.12)。网络荟萃分析表明,与安慰剂相比,P9i+HT、P9i+MT、HT和MT与冠状动脉血运重建和脑血管事件风险降低显著相关。与安慰剂相比,LT可有效降低心血管死亡率(RR 0.71,95%CI 0.54-0.92)、心肌梗死(RR 0.67,95%CI 0.54-0.82)和冠状动脉血运重建(RR 0.77,95%CI 0.65-0.91)的风险。在降低心肌梗死(RR 0.78,95%CI 0.68-0.9)、冠状动脉血运重建(RR 0.84,95%CI 0.73-0.96)和脑血管事件(RR 0.78,95%CI 0.64-0.95)风险方面,P9i+HT优于HT。然而,与安慰剂相比,P9i+HT、HT和MT可增加新发糖尿病风险(分别为RR 1.23,95%CI 1.11-1.37;RR 1.23,95%CI 1.14-1.33;RR 1.09,95%CI 1.02-1.15)。总之,在基础他汀类药物治疗中添加PCSK9i可作为首选降脂治疗推荐,且不会增加新发糖尿病的额外风险。依折麦布的安全性和疗效并不优于他汀类药物。LT可作为初始治疗推荐。