Department of Cardiology, Peking University First Hospital, No. 8, Xishiku Street, Xicheng District, Beijing, 100034, People's Republic of China.
Department of Cardiology, Drum Tower Hospital, Nanjing University Medical School, Nanjing, China.
BMC Anesthesiol. 2021 Nov 9;21(1):276. doi: 10.1186/s12871-021-01496-2.
Treatment decisions in patients undergoing non-cardiac surgery are based on clinical assessment. The Revised Cardiac Risk Index (RCRI) is pragmatic and widely used but has only moderate discrimination. We aimed to test the efficacy of the CHADS-VASc score and the combination of CHADS-VASc and RCRI to predict perioperative risks for non-cardiac surgery.
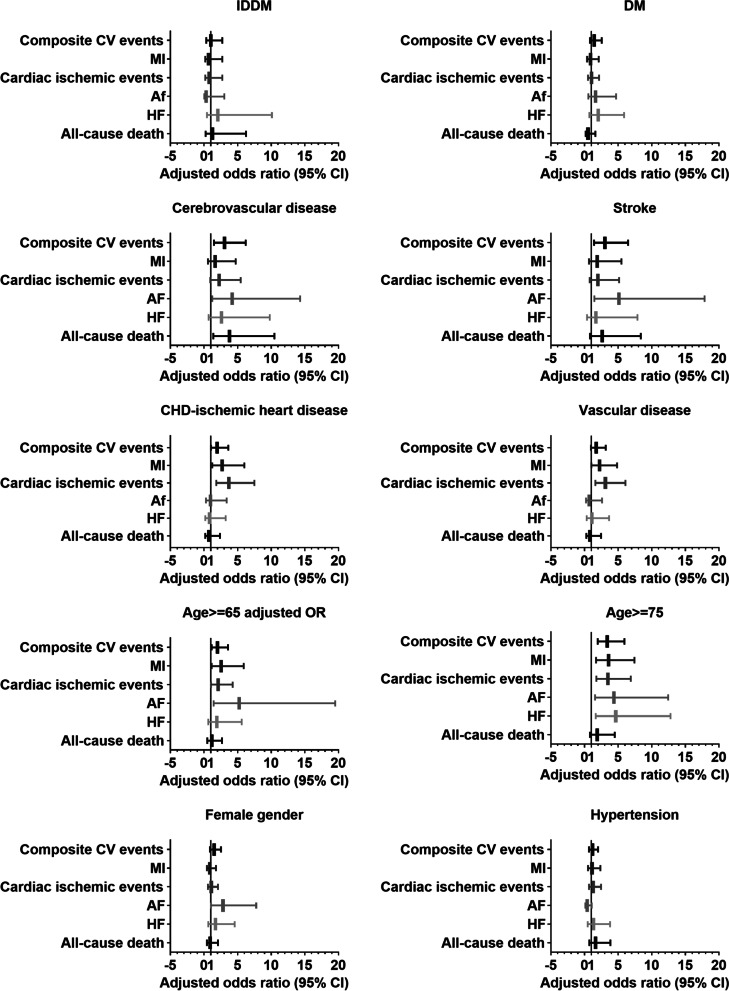
This pre-specified analysis was performed in a retrospective cohort undergoing intra-abdominal surgery in our center from July 1st, 2007 to June 30th, 2008. The possible association between the baseline characteristics (as defined by CHADS-VASc and RCRI) and the primary outcome of composite perioperative cardiac complications (myocardial infarction, cardiac ischemia, heart failure, arrhythmia, stroke, and/or death) and secondary outcomes of individual endpoints were explored using multivariate Logistic regression. The area under the receiver operating characteristic curve (C-statistic) was used for RCRI, CHADS-VASc, and the combined models, and the net reclassification improvement (NRI) was calculated to assess the additional discriminative ability.
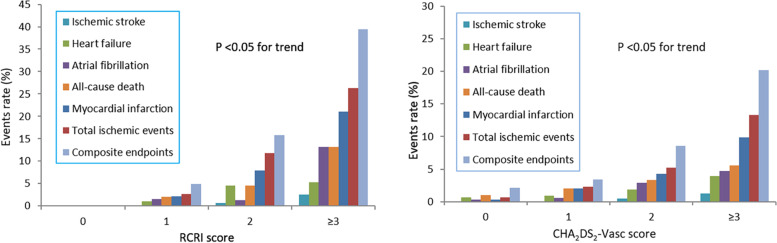
Of the 1079 patients (age 57.5 ± 17.0 years), 460 (42.6%) were women. A total of 83 patients (7.7%) reached the primary endpoint. Secondary outcomes included 52 cardiac ischemic events, 40 myocardial infarction, 20 atrial fibrillation, 18 heart failure, four strokes, and 30 deaths. The endpoint events increased with the RCRI and CHADS-VASc grade elevated (P < 0.05 for trend). The RCRI showed a moderate predictive ability with a C-statistics of 0.668 (95%CI 0.610-0.725) for the composite cardiac outcome. The C-statistics for the CHADS-VASc was 0.765 (95% CI 0.709-0.820), indicating better performance than the RCRI (p = 0.011). Adding the CHADS-VASc to the RCRI further increased the C-statistic to 0.774(95%CI 0.719-0.829), improved sensitivity, negative predictive value, and enhanced reclassification in reference to RCRI. Similar performance of the combined scores was demonstrated in the analysis of individual secondary endpoints. The best cut-off of a total of 4 scores was suggested for the combined CHADS-VASc and RCRI in the prediction of the perioperative cardiac outcomes.
The CHADS-VASc score significantly enhanced risk assessment for the composite perioperative cardiovascular outcome in comparison to traditional RCRI risk stratification. Incorporation of CHADS-VASc scores into clinical-decision making to improve perioperative management in patients undergoing non-cardiac surgery warrants consideration.
非心脏手术患者的治疗决策基于临床评估。修订后的心脏风险指数(RCRI)实用且应用广泛,但具有中等的区分能力。我们旨在检验 CHADS-VASc 评分和 CHADS-VASc 与 RCRI 联合预测非心脏手术围手术期风险的疗效。
本研究为回顾性队列研究,对 2007 年 7 月 1 日至 2008 年 6 月 30 日期间在我院接受腹部手术的患者进行了分析。使用多变量 Logistic 回归分析了基线特征(由 CHADS-VASc 和 RCRI 定义)与主要复合围手术期心脏并发症(心肌梗死、心脏缺血、心力衰竭、心律失常、卒中和/或死亡)和次要终点的各个结局之间的可能关联。使用受试者工作特征曲线下面积(C 统计量)评估 RCRI、CHADS-VASc 和联合模型,计算净重新分类改善(NRI)以评估额外的区分能力。
在 1079 例患者(年龄 57.5±17.0 岁)中,460 例(42.6%)为女性。共有 83 例(7.7%)达到了主要终点。次要结局包括 52 例心脏缺血事件、40 例心肌梗死、20 例心房颤动、18 例心力衰竭、4 例卒中和 30 例死亡。终点事件随 RCRI 和 CHADS-VASc 分级升高而增加(趋势 P<0.05)。RCRI 对复合心脏结局的预测能力中等,C 统计量为 0.668(95%CI 0.610-0.725)。CHADS-VASc 的 C 统计量为 0.765(95%CI 0.709-0.820),表明其性能优于 RCRI(p=0.011)。将 CHADS-VASc 加入 RCRI 后,C 统计量进一步提高至 0.774(95%CI 0.719-0.829),提高了敏感性、阴性预测值,并相对于 RCRI 增强了重新分类。在分析各次要终点时,联合评分也表现出类似的性能。在预测围手术期心脏结局时,建议将 CHADS-VASc 和 RCRI 的总评分设置为 4 分作为最佳截断值。
与传统的 RCRI 风险分层相比,CHADS-VASc 评分显著提高了复合围手术期心血管结局的风险评估。将 CHADS-VASc 评分纳入临床决策以改善非心脏手术患者的围手术期管理值得考虑。