Centre for Translational Medicine, Department of Medicine, University of Szeged, Szeged, Hungary.
Institute for Translational Medicine, Medical School, University of Pécs, Pécs, Hungary.
Eur J Pain. 2022 Mar;26(3):610-623. doi: 10.1002/ejp.1885. Epub 2021 Nov 16.
Pain is the most common symptom in acute pancreatitis (AP) and is among the diagnostic criteria. Therefore, we aimed to characterize acute abdominal pain in AP.
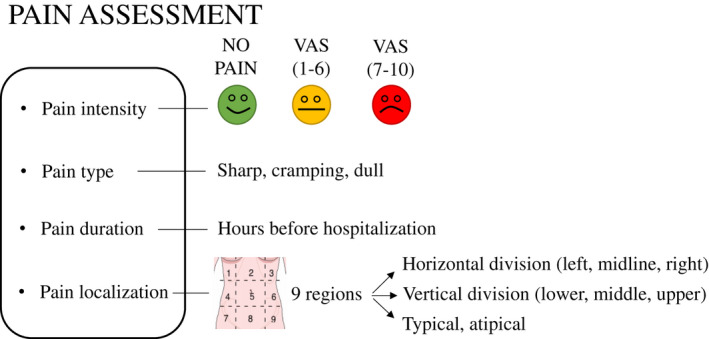
The Hungarian Pancreatic Study Group prospectively collected multicentre clinical data on 1435 adult AP patients between 2012 and 2017. Pain was characterized by its intensity (mild or intense), duration prior to admission (hours), localization (nine regions of the abdomen) and type (sharp, dull or cramping).
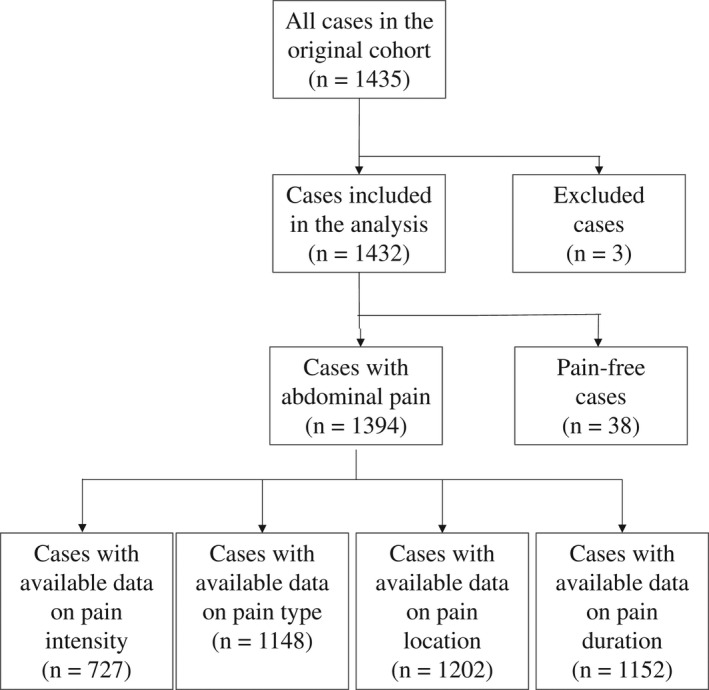
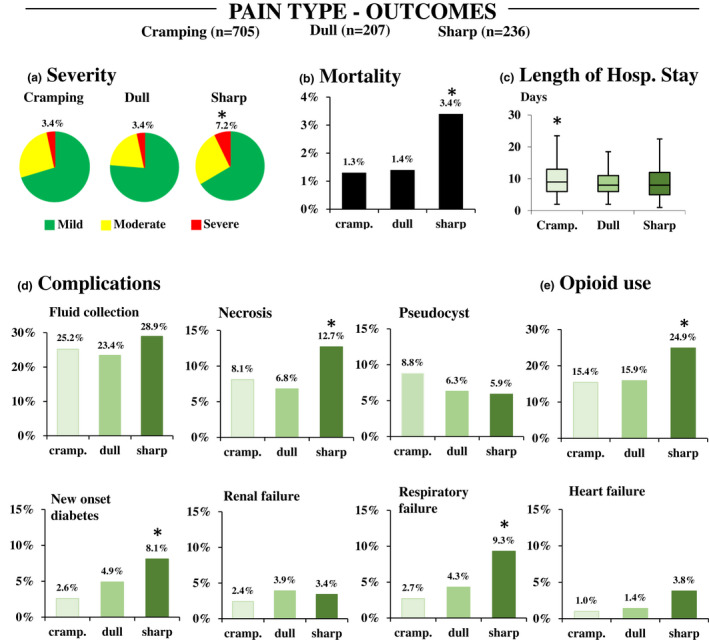
97.3% of patients (n = 1394) had pain on admission. Of the initial population with acute abdominal pain, 727 patients answered questions about pain intensity, 1148 about pain type, 1134 about pain localization and 1202 about pain duration. Pain was mostly intense (70%, n = 511/727), characterized by cramping (61%, n = 705/1148), mostly starting less than 24 h prior to admission (56.7%, n = 682/1202). Interestingly, 50.9% of the patients (n = 577/1134) had atypical pain, which means pain other than epigastric or belt-like upper abdominal pain. We observed a higher proportion of peripancreatic fluid collection (19.5% vs. 11.0%; p = 0.009) and oedematous pancreas (8.4% vs. 3.1%; p = 0.016) with intense pain. Sharp pain was associated with AP severity (OR = 2.481 95% CI: 1.550-3.969) and increased mortality (OR = 2.263, 95% CI: 1.199-4.059) compared to other types. Longstanding pain (>72 h) on admission was not associated with outcomes. Pain characteristics showed little association with the patient's baseline characteristics.
A comprehensive patient interview should include questions about pain characteristics, including pain type. Patients with sharp and intense pain might need special monitoring and tailored pain management.
Acute abdominal pain is the leading presenting symptom in acute pancreatitis; however, we currently lack specific guidelines for pain assessment and management. In our cohort analysis, intense and sharp pain on admission was associated with higher odds for severe AP and several systemic and local complications. Therefore, a comprehensive patient interview should include questions about pain characteristics and patients with intense and sharp pain might need closer monitoring.
疼痛是急性胰腺炎(AP)最常见的症状,也是诊断标准之一。因此,我们旨在描述 AP 患者的急性腹痛特征。
匈牙利胰腺研究组前瞻性收集了 2012 年至 2017 年间 1435 名成年 AP 患者的多中心临床数据。疼痛的特征包括强度(轻度或重度)、入院前持续时间(小时)、定位(腹部九个区域)和类型(锐痛、钝痛或绞痛)。
97.3%(n=1394)的患者入院时存在疼痛。在最初有急性腹痛的人群中,727 名患者回答了关于疼痛强度的问题,1148 名回答了关于疼痛类型的问题,1134 名回答了关于疼痛定位的问题,1202 名回答了关于疼痛持续时间的问题。疼痛大多为重度(70%,n=511/727),表现为绞痛(61%,n=705/1148),大多在入院前不到 24 小时开始(56.7%,n=682/1202)。有趣的是,50.9%(n=577/1134)的患者存在非典型疼痛,即上腹部非剑突下或腰带样疼痛。我们观察到重度疼痛患者的胰周液体积聚(19.5%比 11.0%;p=0.009)和水肿性胰腺炎(8.4%比 3.1%;p=0.016)比例较高。与其他类型相比,锐痛与 AP 严重程度(比值比=2.481,95%置信区间:1.550-3.969)和死亡率增加(比值比=2.263,95%置信区间:1.199-4.059)相关。入院时持续疼痛(>72 小时)与结局无关。疼痛特征与患者的基线特征几乎没有关联。
全面的患者访谈应包括疼痛特征的问题,包括疼痛类型。入院时出现锐痛和重度疼痛的患者可能需要特殊监测和针对性的疼痛管理。
急性腹痛是急性胰腺炎的主要首发症状;然而,我们目前缺乏疼痛评估和管理的具体指南。在我们的队列分析中,入院时的重度和锐痛与更严重的 AP 以及多种全身和局部并发症的发生几率较高相关。因此,全面的患者访谈应包括疼痛特征的问题,而入院时存在重度和锐痛的患者可能需要更密切的监测。