Thyavihally Yuvaraja B, Waigankar Santosh S, Dev Preetham, Asari Ashish, Pednekar Abhinav P, Athikari Nevitha, Raut Abhijit, Khandekar Archan, Badlani Naresh
Department of Uro-Oncology, Kokilaben Dhirubhai Ambani Hospital and Research Institute, Mumbai, Maharashtra, India.
Department of Pathology, Kokilaben Dhirubhai Ambani Hospital and Research Institute, Mumbai, Maharashtra, India.
Urol Ann. 2021 Oct-Dec;13(4):424-430. doi: 10.4103/UA.UA_139_20. Epub 2021 Sep 2.
The recommended treatment for intermediate and high-risk nonmuscle invasive bladder cancer (NMIBC) is adjuvant intravesical bacillus Calmette-Guerin (BCG) instillation. However, up to 50% experience tumor recurrences even after adjuvant BCG, and many patients develop local or systemic adverse effects. Our study compared adverse effects, short-term recurrence rates, and cost-implications of BCG therapy to Hyperthermic Intra-VEsical Chemotherapy (HIVEC) with Mitomycin-C (MMC) in these patients.
Retrospective analysis of intermediate and high-risk NMIBC patients who received either intravesical BCG or HIVEC after transurethral resection of bladder tumor in our institute (January 2017 to March 2020) was done. Twenty-two patients who received HIVEC and 29 who received BCG were analyzed. We used SPSS Statistics v20.0 (IBM Corp., Armonk, NY, USA) software for the statistical analysis.
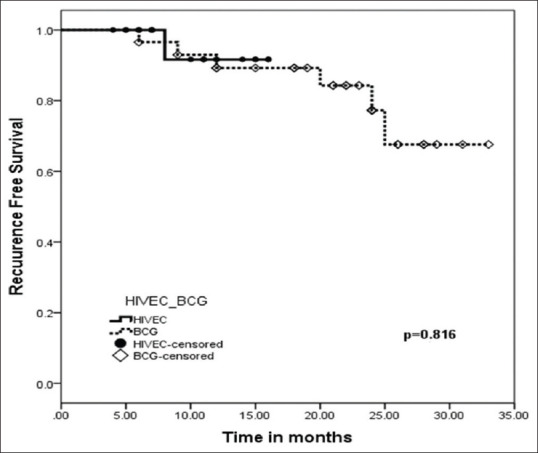
Nineteen (86.4%) patients in the HIVEC group had no adverse effects. Two (9.1%) patients had Grade I lower urinary tract symptoms (LUTS) treated symptomatically. One patient developed UTI after HIVEC, and further cycles were stopped (Grade II). BCG group had a higher rate of Grade III adverse effects in six (20.7%) patients. Median follow-up was 10.5 and 22 months. The tumor recurred in one (4.5%) and six (20.7%) patients in HIVEC and BCG groups, respectively. There was no difference in recurrence-free survival at 18 months and the cost for the HIVEC therapy was more.
HIVEC with MMC is a reasonable adjuvant treatment option in NMIBC, which is well tolerated, albeit increased cost of the treatment. Randomized trials with more follow-up are required for further conclusion.
中高危非肌层浸润性膀胱癌(NMIBC)的推荐治疗方法是辅助性膀胱内灌注卡介苗(BCG)。然而,即使在辅助性BCG治疗后,仍有高达50%的患者出现肿瘤复发,且许多患者会出现局部或全身不良反应。我们的研究比较了BCG治疗与丝裂霉素C(MMC)热灌注膀胱化疗(HIVEC)对这些患者的不良反应、短期复发率和成本影响。
对我院2017年1月至2020年3月期间经尿道膀胱肿瘤切除术后接受膀胱内BCG或HIVEC治疗的中高危NMIBC患者进行回顾性分析。分析了22例接受HIVEC治疗的患者和29例接受BCG治疗的患者。我们使用SPSS Statistics v20.0(美国纽约州阿蒙克市IBM公司)软件进行统计分析。
HIVEC组19例(86.4%)患者无不良反应。2例(9.1%)患者出现I级下尿路症状(LUTS),经对症治疗。1例患者在HIVEC治疗后发生尿路感染,后续疗程停止(II级)。BCG组有6例(20.7%)患者出现III级不良反应的发生率较高。中位随访时间分别为10.5个月和22个月。HIVEC组和BCG组分别有1例(4.5%)和6例(20.7%)患者肿瘤复发。18个月时无复发生存率无差异,且HIVEC治疗费用更高。
MMC的HIVEC是NMIBC中一种合理的辅助治疗选择,耐受性良好,尽管治疗成本增加。需要进行更多随访的随机试验以得出进一步结论。