Department of Intensive Medicine, Hebei General Hospital, Shijiazhuang City, Hebei Province, P.R. China.
Department of Orthopaedics Surgery, Children's Hospital of Hebei, Shijiazhuang City, Hebei Province, P.R. China.
Medicine (Baltimore). 2021 Nov 19;100(46):e27896. doi: 10.1097/MD.0000000000027896.
Amniotic fluid embolism (AFE) is a rare obstetrical complication and is a leading cause of maternal death in developed countries. Despite the development of supportive therapeutic measures, the mortality rate remains high.
A 38-year-old nulliparous pregnant woman, who underwent in vitro fertilization-embryo transfer, was admitted for labor at 37 weeks' gestation. Approximately 30 minutes after delivery of the placenta, the puerpera developed postpartum hemorrhage with uterine atony. Soon after, the patient experienced hypotension, repeated cardiac arrest, refectory hypoxia, and disseminated intravascular coagulopathy.
AFE is diagnosed clinically. The pregnant woman in this case fulfilled the diagnostic criteria for AFE: acute hypotension, cardiac arrest, acute hypoxia, and coagulation disorders within approximately 30 minutes after delivery of the placenta.
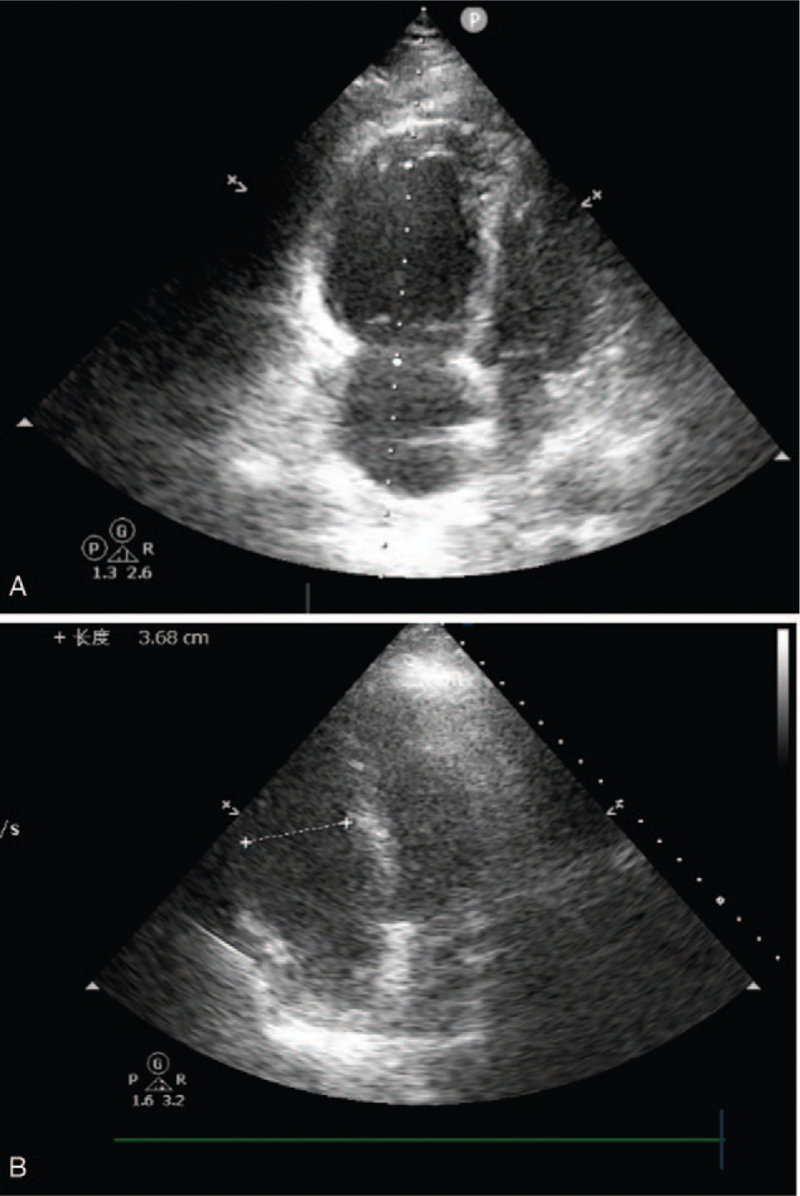
The patient was intubated, connected to a ventilator, and was administered a high dose of vasoactive drugs to maintain blood pressure and underwent an emergency hysterectomy. Considering the risk for recurrent cardiac arrest and severe refractory hypoxia, venoarterial extracorporeal membrane oxygenation was initiated and discontinued as soon as cardiac function was restored based on serial bedside ultrasound assessment.
The patient stabilized on day 7 in the intensive care unit and was transferred to the obstetrics ward and, 1 week later, was discharged with no complications. Two months later, follow-up revealed that the patient was in good condition.
Serial bedside ultrasound was crucial for assessing cardiac function and optimal weaning. Timely application of venoarterial extracorporeal membrane oxygenation and weaning was significant to avoid the occurrence of complications and improve long-term outcomes.
羊水栓塞(AFE)是一种罕见的产科并发症,也是发达国家产妇死亡的主要原因。尽管支持性治疗措施有所发展,但死亡率仍然很高。
一位 38 岁的初产妇,行体外受精-胚胎移植,妊娠 37 周入院分娩。胎盘娩出后约 30 分钟,产妇发生产后出血伴子宫收缩乏力。随后,患者出现低血压、反复心脏骤停、反射性缺氧和弥散性血管内凝血。
临床诊断为 AFE。本例患者符合 AFE 的诊断标准:胎盘娩出后约 30 分钟内出现急性低血压、心脏骤停、急性缺氧和凝血功能障碍。
患者行气管插管、呼吸机辅助通气,并给予大剂量血管活性药物维持血压,行急症子宫切除术。考虑到再次心脏骤停和严重难治性缺氧的风险,在床边连续超声评估后,一旦心脏功能恢复,即开始并停止静脉-动脉体外膜肺氧合。
患者在重症监护病房第 7 天稳定,转至产科病房,1 周后无并发症出院。2 个月后随访显示患者状况良好。
床边连续超声对评估心功能和最佳脱机至关重要。及时应用静脉-动脉体外膜肺氧合和脱机对避免并发症发生和改善长期预后具有重要意义。