Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
Department of Surgery, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
Thorac Cancer. 2022 Jan;13(2):182-189. doi: 10.1111/1759-7714.14237. Epub 2021 Nov 20.
Although epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) have been the standard treatment for advanced EGFR-mutant adenocarcinoma, the effects of upfront EGFR-TKI use in unresectable stage III EGFR-mutant adenocarcinoma remain unexplored. Here, we conducted a retrospective study to compare different treatment strategies in these patients.
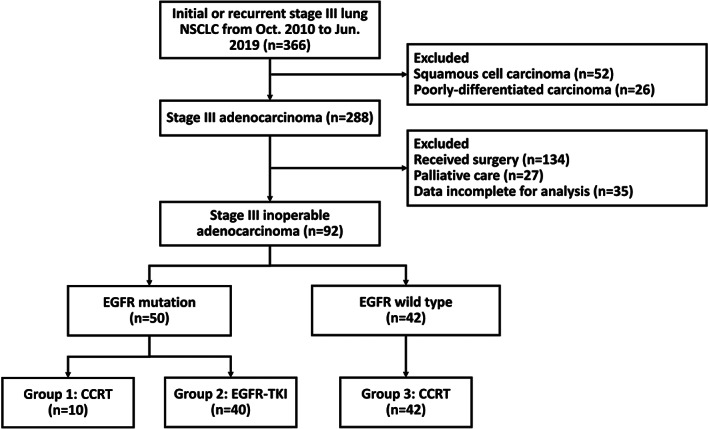
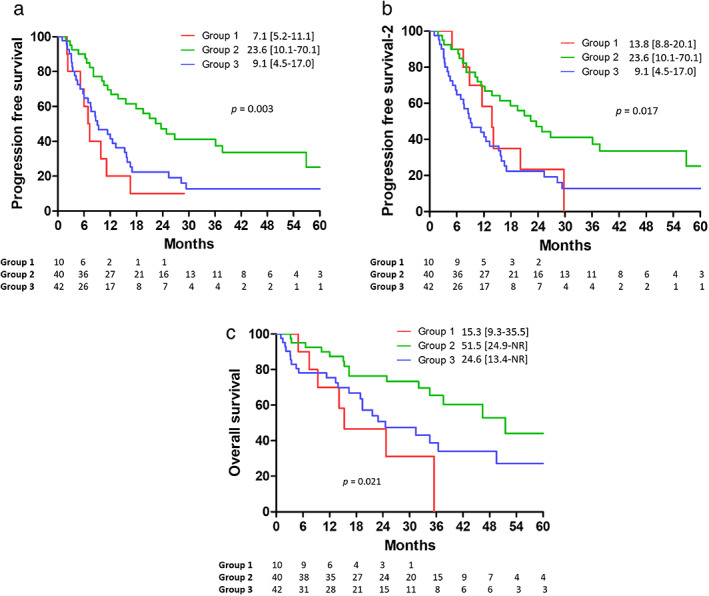
From October 2010 to June 2019, patients with unresectable stage III adenocarcinoma who received treatment at a tertiary referral center were enrolled. Patients were classified into three groups: EGFR-mutant adenocarcinoma treated with concurrent chemoradiotherapy (group 1) or EGFR-TKI (group 2) and EGFR wild-type adenocarcinoma treated with concurrent chemoradiotherapy (group 3). Progression-free survival, progression-free survival-2, and overall survival were estimated and compared using Kaplan-Meier and log-rank tests.
A total of 92 patients were enrolled; 10, 40, and 42 patients were assigned to groups 1, 2, and 3, respectively. Patients with EGFR mutations who received upfront EGFR-TKIs had significantly longer progression-free and overall survival than those who received upfront concurrent chemoradiotherapy (hazard ratio 0.33 vs. 0.34, p = 0.006 vs. 0.031) according to a Cox model adjusted for possible confounders. Moreover, upfront concurrent chemoradiotherapy did not lead to higher survival rates in patients with EGFR mutations than in those with EGFR wild-type adenocarcinoma (progression-free survival; hazard ratio 0.37, p = 0.036; overall survival; hazard ratio 0.35, p = 0.080) by Cox regression analysis.
This current study suggests that EGFR-TKIs is a better choice for patients with unresectable stage III EGFR-mutant adenocarcinoma. However, further randomized studies are required to validate the results.
尽管表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKIs)已成为晚期 EGFR 突变型腺癌的标准治疗方法,但在不可切除的 III 期 EGFR 突变型腺癌中, upfront EGFR-TKI 的使用效果仍未得到探索。在这里,我们进行了一项回顾性研究,以比较这些患者的不同治疗策略。
从 2010 年 10 月至 2019 年 6 月,在一家三级转诊中心接受治疗的不可切除的 III 期腺癌患者被纳入研究。患者被分为三组:接受同步放化疗(组 1)或 EGFR-TKI(组 2)治疗的 EGFR 突变型腺癌患者和接受同步放化疗(组 3)治疗的 EGFR 野生型腺癌患者。使用 Kaplan-Meier 和对数秩检验估计和比较无进展生存期、无进展生存期-2 和总生存期。
共纳入 92 例患者;分别有 10、40 和 42 例患者被分配到组 1、组 2 和组 3。根据 Cox 模型调整可能的混杂因素后, upfront EGFR-TKIs 治疗的 EGFR 突变患者的无进展生存期和总生存期显著长于 upfront 同步放化疗患者(风险比 0.33 对 0.34,p=0.006 对 0.031)。此外, Cox 回归分析显示, upfront 同步放化疗并未导致 EGFR 突变患者的生存率高于 EGFR 野生型腺癌患者(无进展生存期;风险比 0.37,p=0.036;总生存期;风险比 0.35,p=0.080)。
本研究表明,EGFR-TKIs 是不可切除的 III 期 EGFR 突变型腺癌患者的更好选择。然而,需要进一步的随机研究来验证这些结果。