Masiá Mar, Padilla Sergio, García José Alberto, García-Abellán Javier, Navarro Andrés, Guillén Lucía, Telenti Guillermo, Mascarell Paula, Botella Ángela, Gutiérrez Félix
Infectious Diseases Unit, Hospital General Universitario de Elche, Universidad Miguel Hernández, Elche, Spain.
Infectious Diseases Unit, Hospital General Universitario de Elche, Elche, Spain.
Front Med (Lausanne). 2021 Nov 8;8:749657. doi: 10.3389/fmed.2021.749657. eCollection 2021.
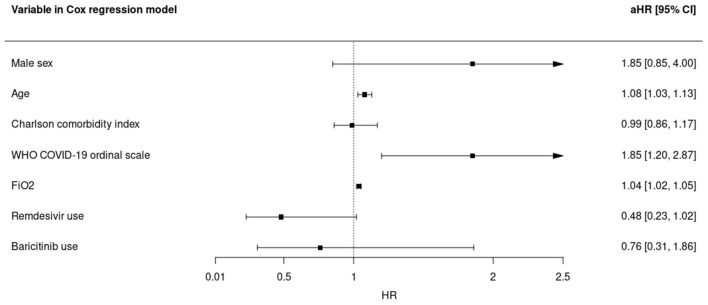
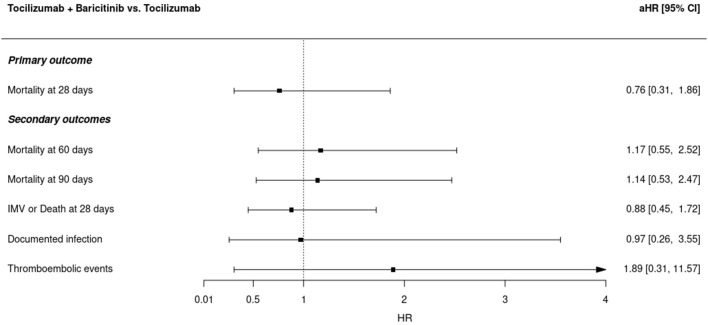
Baricitinib is a Janus kinase (JAK) inhibitor with a broader anti-inflammatory activity than tocilizumab and an antiviral potential although no head-to-head trials are available. The benefits of adding baricitinib to patients with COVID-19 experiencing clinical progression despite the standard of care (SOC), including corticosteroids and tocilizumab, are also unknown. A cohort study included microbiologically confirmed COVID-19 hospitalizations. The primary outcome was 28-day mortality. Secondary outcomes were 60- and 90-day mortality, the composite outcome "28-day invasive mechanical ventilation (IMV) or death" and the safety of the combination. Propensity score (PS) matching was used to identify the association between baricitinib use and the outcomes of interest. Of 1,709 admissions, 994 patients received corticosteroids and tocilizumab and 110 of them received baricitinib after tocilizumab. PS matched 190 (95:95) patients with baricitinib + SOC vs. SOC, of whom 69.5% received remdesivir. No significant effect of baricitinib was observed on 28-day [39 events; adjusted hazard ratio (aHR), 0.76; 95% CI, 0.31-1.86], 60-day (49 events, aHR, 1.17; 95% CI, 0.55-2.52), or 90-day mortality (49 events; aHR, 1.14; 95% CI, 0.53-2.47), or on the composite outcome 28-day IMV/death (aHR, 0.88; 95% CI, 0.45-1.72). Secondary infections during hospitalization were not different between groups (17.9 vs. 10.5%, respectively; = 0.212) and thromboembolic events were higher with baricitinib (11.6% vs. 3.2%; = 0.048), but differences vanished after the adjustment [aHR 1.89 (0.31-11.57), = 0.490]. The addition of baricitinib did not substantially reduce mortality in hospitalized patients with COVID-19 having clinical progression despite the therapy with tocilizumab and corticosteroids. The combination of baricitinib and tocilizumab was not associated with an increased risk of secondary infections or thromboembolic events.
巴瑞替尼是一种Janus激酶(JAK)抑制剂,与托珠单抗相比具有更广泛的抗炎活性,并且具有抗病毒潜力,尽管尚无直接对比试验。对于尽管接受了包括皮质类固醇和托珠单抗在内的标准治疗(SOC)但病情仍在临床进展的COVID-19患者,加用巴瑞替尼的益处也尚不清楚。一项队列研究纳入了微生物学确诊的COVID-19住院患者。主要结局是28天死亡率。次要结局是60天和90天死亡率、复合结局“28天有创机械通气(IMV)或死亡”以及联合用药的安全性。采用倾向评分(PS)匹配来确定使用巴瑞替尼与感兴趣结局之间的关联。在1709例入院患者中,994例患者接受了皮质类固醇和托珠单抗治疗,其中110例在使用托珠单抗后接受了巴瑞替尼治疗。PS匹配了190例(95:95)接受巴瑞替尼+SOC与仅接受SOC治疗的患者,其中69.5%的患者接受了瑞德西韦治疗。未观察到巴瑞替尼对28天死亡率(39例事件;调整后风险比[aHR],0.76;95%置信区间[CI],0.31 - 1.86)、60天死亡率(49例事件,aHR,1.17;95%CI,0.55 - 2.52)或90天死亡率(49例事件;aHR,1.14;95%CI,0.53 - 2.47),或对复合结局28天IMV/死亡(aHR,0.88;95%CI,0.45 - 1.72)有显著影响。住院期间的继发感染在两组之间无差异(分别为17.9%和10.5%;P = 0.212),巴瑞替尼组的血栓栓塞事件发生率更高(11.6%对3.2%;P = 0.048),但调整后差异消失[aHR 1.89(0.31 - 11.57),P = 0.490]。对于尽管接受了托珠单抗和皮质类固醇治疗但仍有临床进展的COVID-19住院患者,加用巴瑞替尼并未显著降低死亡率。巴瑞替尼与托珠单抗联合使用与继发感染或血栓栓塞事件风险增加无关。