Guimarães Tales Mollica, Giglio Pedro Nogueira, Sobrado Marcel Faraco, Bonadio Marcelo Batista, Gobbi Riccardo Gomes, Pécora José Ricardo, Helito Camilo Partezani
Grupo de Joelho, Instituto de Ortopedia e Traumatologia, Hospital das Clínicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil.
Hospital Sírio Libanês, São Paulo, Brazil.
Orthop J Sports Med. 2021 Nov 17;9(11):23259671211056325. doi: 10.1177/23259671211056325. eCollection 2021 Nov.
The degree of knee hyperextension in isolation has not been studied in detail as a risk factor that could lead to increased looseness or graft failure after anterior cruciate ligament (ACL) reconstruction.
To analyze whether more than 5° of passive knee hyperextension is associated with worse functional outcomes and greater risk of graft failure after primary ACL reconstruction with hamstring tendon autograft.
Cohort study; Level of evidence, 3.
A cohort of patients who had primary ACL reconstruction with hamstring tendon autografts was divided into 2 groups based on passive contralateral knee hyperextension greater than 5° (hyperextension group) and less than 5° (control group) of hyperextension. Groups were matched by age, sex, and associated meniscal tears. The following data were collected and compared between the groups: patient data (age and sex), time from injury to surgery, passive knee hyperextension, KT-1000 arthrometer laxity, pivot shift, associated meniscal injury and treatment (meniscectomy or repair), contralateral knee ligament injury, intra-articular graft size, follow-up time, occurrence of graft failure, and postoperative Lysholm knee scale and International Knee Documentation Committee subjective form scores.
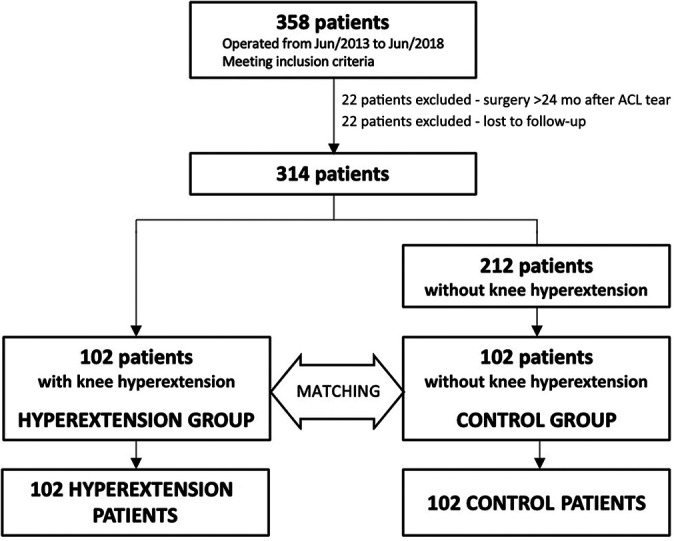
Data from 358 patients initially included in the study were analyzed; 22 were excluded because the time from injury to surgery was greater than 24 months, and 22 were lost to follow-up. From the cohort of 314 patients, 102 had more than 5° of knee hyperextension. A control group of the same size (n = 102) was selected by matching among the other 212 patients. Significant differences in the incidence of graft failure (14.7% vs 2.9%; = .005) and Lysholm knee scale score (86.4 ± 9.8 vs 89.6 ± 6.1; = .018) were found between the 2 groups.
Patients with more than 5° of contralateral knee hyperextension submitted to single-bundle ACL reconstruction with hamstring tendons have a higher failure rate than patients with less than 5° of knee hyperextension.
单纯膝关节过伸程度作为前交叉韧带(ACL)重建术后导致松动增加或移植物失败的危险因素尚未得到详细研究。
分析在自体腘绳肌腱初次ACL重建术后,被动膝关节过伸超过5°是否与更差的功能结果及更高的移植物失败风险相关。
队列研究;证据等级,3级。
将一组接受自体腘绳肌腱初次ACL重建的患者,根据对侧膝关节被动过伸大于5°(过伸组)和小于5°(对照组)分为两组。两组在年龄、性别和相关半月板撕裂情况方面进行匹配。收集并比较两组间以下数据:患者资料(年龄和性别)、受伤至手术时间、膝关节被动过伸、KT-1000关节测压计松弛度、轴移试验、相关半月板损伤及治疗(半月板切除术或修复)、对侧膝关节韧带损伤、关节内移植物大小、随访时间、移植物失败发生率以及术后Lysholm膝关节评分和国际膝关节文献委员会主观评分表得分。
对最初纳入研究的358例患者的数据进行分析;22例因受伤至手术时间大于24个月被排除,22例失访。在314例患者队列中,102例膝关节过伸超过5°。通过在其他212例患者中进行匹配,选取了相同规模的对照组(n = 102)。两组间移植物失败发生率(14.7%对2.9%;P = 0.005)和Lysholm膝关节评分(86.4±9.8对89.6±6.1;P = 0.018)存在显著差异。
接受单束腘绳肌腱ACL重建且对侧膝关节过伸超过5°的患者,比膝关节过伸小于5°的患者失败率更高。