Lissat Andrej, van Schewick Claudia, Steffen Ingo G, Arakawa Ayumu, Bourquin Jean-Pierre, Burkhardt Birgit, Henze Guenter, Mann Georg, Peters Christina, Sramkova Lucie, Eckert Cornelia, von Stackelberg Arend, Chen-Santel Christiane
Department of Pediatric Hematology and Oncology, Charité-Universitätsmedizin Berlin, Augstenburger Platz 1, 13353 Berlin, Germany.
Eleonoren-Foundation, Pediatric Hematology Oncology Department, University Children's Hospital Zürich, Steinwiesstraße 75, CH-8032 Zürich, Switzerland.
J Clin Med. 2021 Nov 14;10(22):5292. doi: 10.3390/jcm10225292.
Children with other extramedullary relapse of acute lymphoblastic leukemia are currently poorly characterized. We aim to assess the prevalence and the clinical, therapeutic and prognostic features of extramedullary localizations other than central nervous system or testis in children with relapse of acute lymphoblastic leukemia (ALL) and lymphoblastic lymphoma (LBL) treated on a relapsed ALL protocol.
Patients with relapse of ALL and LBL, treated according to the multicentric ALL-REZ BFM trials between 1983 and 2015, were analyzed for other extramedullary relapse (OEMR) of the disease regarding clinical features, treatment and outcome. Local treatment/irradiation has been recommended on an individual basis and performed only in a minority of patients.
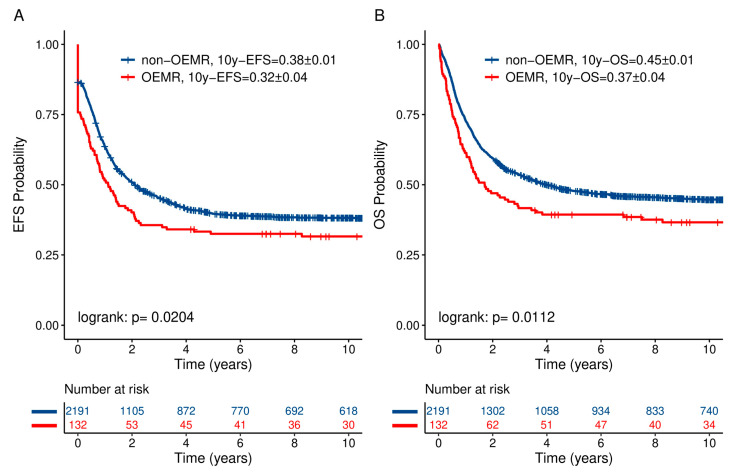
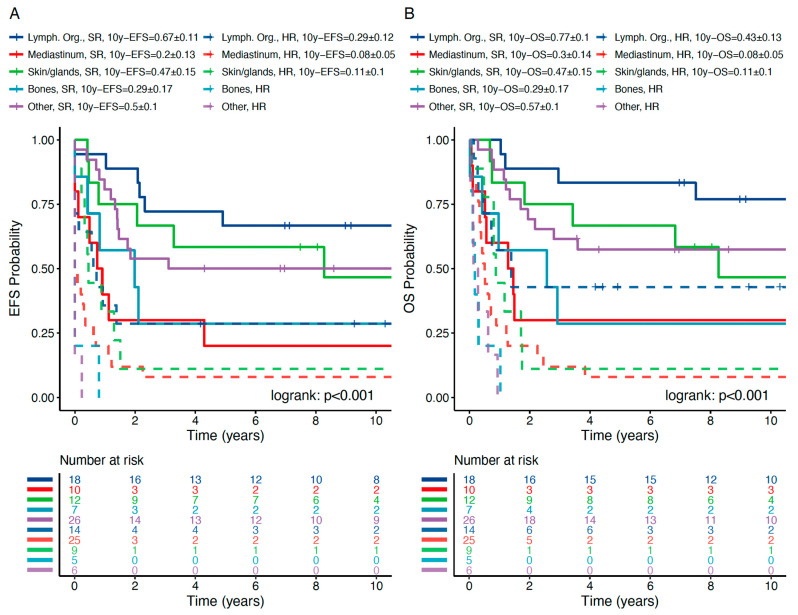
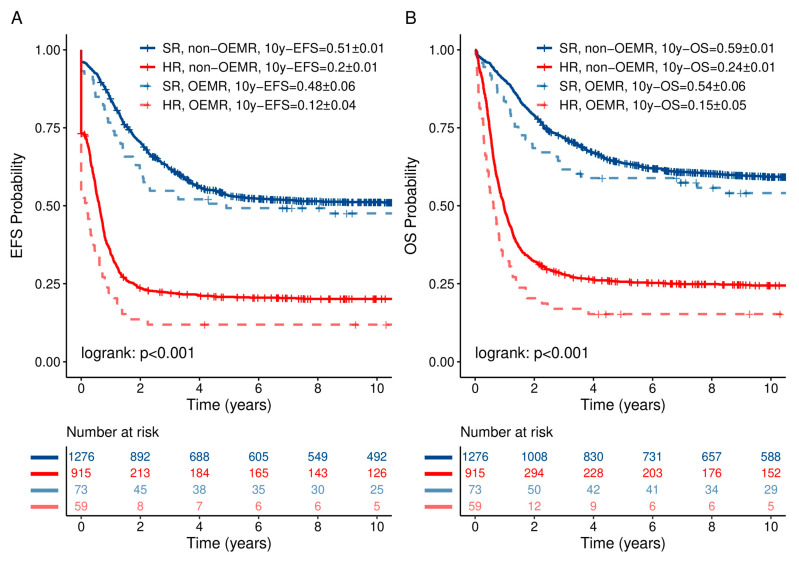
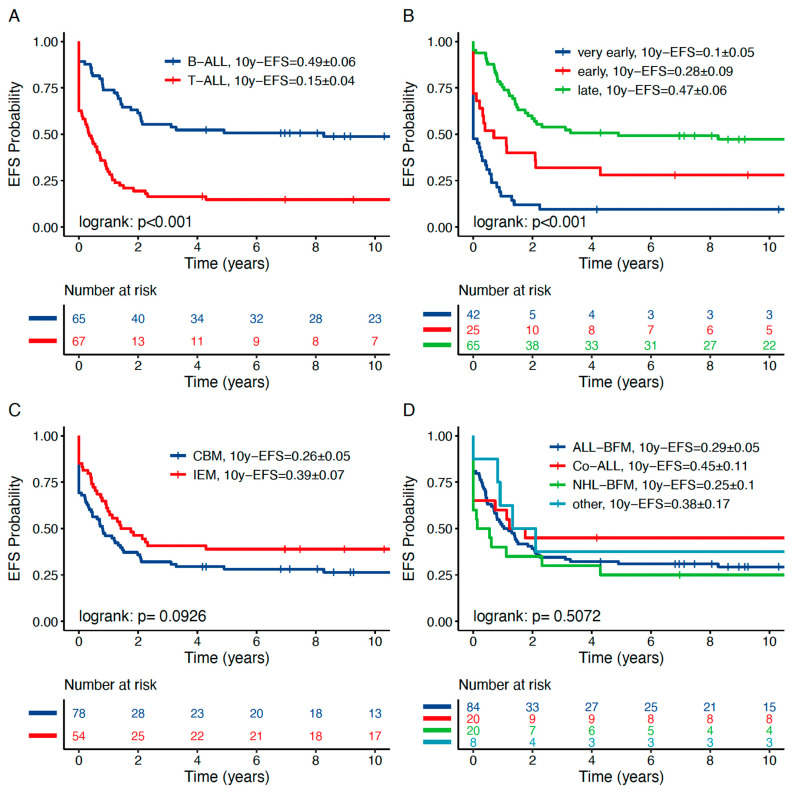
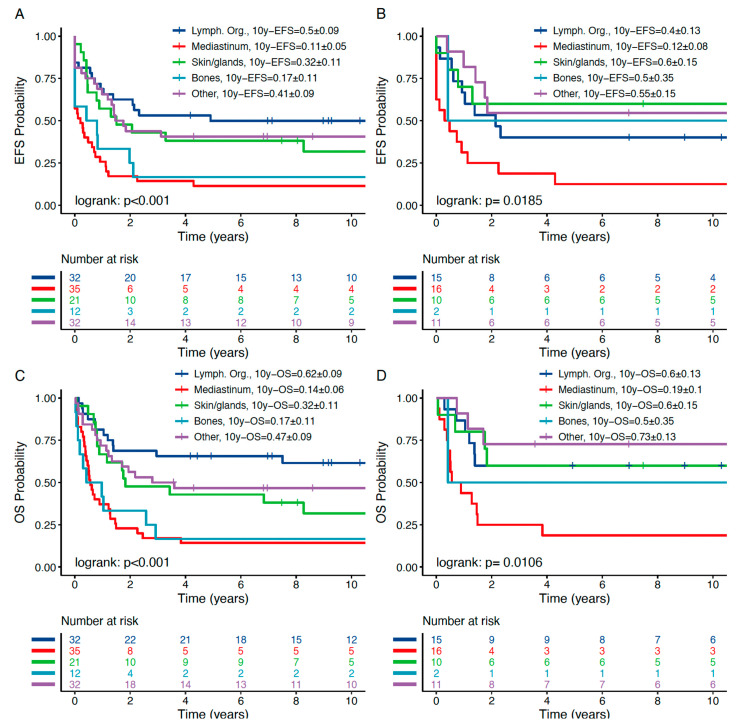
A total of 132 out of 2323 (5.6%) patients with ALL relapse presented with an OEMR (combined bone marrow relapse = 78; isolated extramedullary relapse = 54). Compared to the non-OEMR group, patients with OEMR had a higher rate of T-immunophenotype ( < 0.001), a higher rate of LBL ( < 0.001) and a significantly different distribution of time to relapse, i.e., more very early and late relapses compared to the non-OEMR group ( = 0.01). Ten-year probabilities of event-free survival (pEFS) and overall survival (pOS) in non-OEMR vs. OEMR were 0.38 ± 0.01 and 0.32 ± 0.04 ( = 0.0204) vs. 0.45 ± 0.01 and 0.37 ± 0.04 ( = 0.0112), respectively. OEMRs have been classified into five subgroups according to the main affected compartment: lymphatic organs ( = 32, 10y-pEFS 0.50 ± 0.09), mediastinum ( = 35, 10y-pEFS 0.11 ± 0.05), bone ( = 12, 0.17 ± 0.11), skin and glands ( = 21, 0.32 ± 0.11) and other localizations ( = 32, 0.41 ± 0.09). Patients with OEMR and T-lineage ALL/LBL showed a significantly worse 10y-pEFS (0.15 ± 0.04) than those with B-Precursor-ALL (0.49 ± 0.06, < 0.001). Stratified into standard risk (SR) and high risk (HR) groups, pEFS and pOS of OEMR subgroups were in the expected range whereas the mediastinal subgroup had a significantly worse outcome. Subsequent relapses involved more frequently the bone marrow (58.4%) than isolated extramedullary compartments (41.7%). In multivariate Cox regression, OEMR confers an independent prognostic factor for inferior pEFS and pOS.
OEMR is adversely related to prognosis. However, the established risk classification can be applied for all subgroups except mediastinal relapses requiring treatment intensification. Generally, isolated OEMR of T-cell-origin needs an intensified treatment including allogeneic stem cell transplantation (HSCT) as a curative approach independent from time to relapse. Local therapy such as surgery and irradiation may be of benefit in selected cases. The indication needs to be clarified in further investigations.
目前,急性淋巴细胞白血病其他髓外复发的儿童特征尚不明确。我们旨在评估接受复发性急性淋巴细胞白血病(ALL)方案治疗的急性淋巴细胞白血病(ALL)和淋巴细胞淋巴瘤(LBL)复发患儿中,除中枢神经系统或睾丸外的髓外定位的患病率、临床、治疗和预后特征。
分析1983年至2015年间根据多中心ALL-REZ BFM试验治疗的ALL和LBL复发患者的疾病其他髓外复发(OEMR)情况,包括临床特征、治疗和结局。已建议根据个体情况进行局部治疗/放疗,且仅在少数患者中进行。
2323例ALL复发患者中有132例(5.6%)出现OEMR(合并骨髓复发 = 78例;孤立性髓外复发 = 54例)。与非OEMR组相比,OEMR患者的T免疫表型率更高(<0.001),LBL率更高(<0.001),复发时间分布显著不同,即与非OEMR组相比,极早期和晚期复发更多(=0.01)。非OEMR组与OEMR组的10年无事件生存率(pEFS)和总生存率(pOS)分别为0.38±0.01和0.32±0.04(=0.0204),以及0.45±0.01和0.37±0.04(=0.0112))。根据主要受累部位,OEMR被分为五个亚组:淋巴器官(=32例,10年pEFS 0.50±0.09)、纵隔(=35例,10年pEFS 0.11±0.05)、骨骼(=12例,0.17±0.11)、皮肤和腺体(=21例,0.32±0.11)以及其他部位(=32例,0.41±0.09)。OEMR和T系ALL/LBL患者的10年pEFS(0.15±0.04)显著低于B前体ALL患者(0.49±0.06,<0.001)。分为标准风险(SR)和高风险(HR)组后,OEMR亚组的pEFS和pOS在预期范围内,而纵隔亚组的结局显著更差。后续复发更频繁累及骨髓(58.4%)而非孤立的髓外部位(41.7%)。在多变量Cox回归中,OEMR是pEFS和pOS较差的独立预后因素。
OEMR与预后呈负相关。然而,既定的风险分类可应用于所有亚组,但纵隔复发需要强化治疗。一般来说,T细胞起源的孤立性OEMR需要强化治疗,包括异基因干细胞移植(HSCT)作为一种独立于复发时间的治愈方法。手术和放疗等局部治疗在某些情况下可能有益。需要在进一步研究中明确适应证。