Division of Dermatology, Department of Medicine, University of Washington, USA.
Division of Dermatology, Department of Medicine, University of Washington, USA; Fred Hutchinson Cancer Research Center, Seattle, USA.
J Dermatol Sci. 2022 Jan;105(1):2-10. doi: 10.1016/j.jdermsci.2021.10.004. Epub 2021 Oct 18.
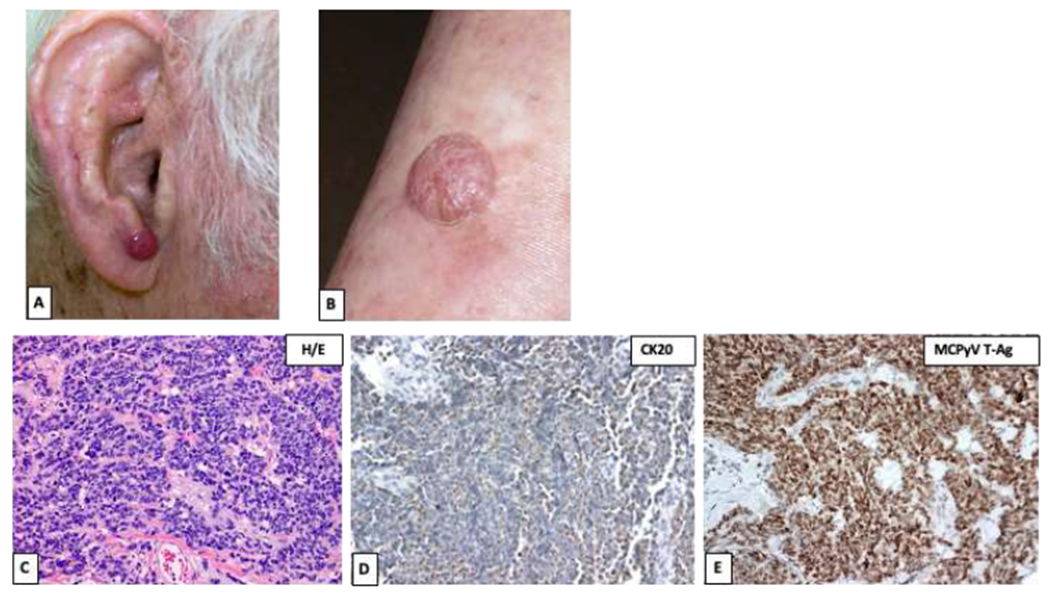
Merkel cell carcinoma (MCC) is a primary neuroendocrine skin cancer that recurs in ~40% of cases. Merkel cell polyomavirus (MCPyV) and ultraviolet (UV)-induced mutations are two major causative factors of MCC. Virus-positive MCCs express polyomavirus oncoproteins that are highly immunogenic yet are required for ongoing tumor growth. Virus-negative MCCs have a high burden of UV-DNA mutations that encode tumor-specific UV-neoantigens. Thus, both UV- and virus-induced MCCs are highly immunogenic, enabling diverse T-cell targeted therapies. Optimal MCC management is challenging given its rarity, aggressive nature, rapidly evolving care guidelines, and fundamental differences in management compared to other skin cancers. MCC is often managed aggressively with extensive surgery, radiotherapy or systemic therapy, frequently leading to toxicities that might have been avoidable while still achieving optimal disease control. Thus, multi-disciplinary care is crucial for providing patients with the best possible outcomes. The outlook for many patients with advanced MCC has progressed remarkably over the past decade due to PD-1 pathway blocking agents that provide durable benefit for a substantial subset of MCC patients. The management of early-stage MCC has also improved due to better approaches to integrate surgery and radiotherapy. Prognostic accuracy and ongoing surveillance have advanced due to stage-specific recurrence data and sophisticated "liquid biopsies" that allow early detection of disease recurrence. Here we summarize both recent striking progress and pressing challenges such as PD-(L)1-refractory MCC, and management of MCC patients with immune dysfunction. We also highlight diverse resources to allow providers to take advantage of recent progress in this fast-moving field.
默克尔细胞癌(Merkel cell carcinoma,MCC)是一种原发性神经内分泌皮肤癌,约有 40%的病例会复发。默克尔细胞多瘤病毒(Merkel cell polyomavirus,MCPyV)和紫外线(ultraviolet,UV)诱导的突变是 MCC 的两个主要致病因素。阳性 MCC 表达多瘤病毒癌蛋白,这些蛋白具有高度免疫原性,但也是肿瘤持续生长所必需的。阴性 MCC 具有大量编码肿瘤特异性 UV-新抗原的 UV-DNA 突变。因此,UV 和病毒诱导的 MCC 都具有高度的免疫原性,能够实现多种针对 T 细胞的治疗方法。鉴于其罕见性、侵袭性、不断演变的治疗指南以及与其他皮肤癌相比在管理方面的根本差异,MCC 的最佳管理极具挑战性。MCC 通常采用广泛的手术、放疗或全身治疗进行积极治疗,经常导致毒性反应,这些毒性反应在仍能实现最佳疾病控制的情况下可能是可以避免的。因此,多学科护理对于为患者提供最佳结果至关重要。由于 PD-1 通路阻断剂为大量 MCC 患者提供了持久的益处,过去十年中,许多晚期 MCC 患者的预后有了显著改善。由于更好的方法可以整合手术和放疗,早期 MCC 的治疗也得到了改善。由于具有特定阶段的复发数据和复杂的“液体活检”,可以早期发现疾病复发,因此预后准确性和持续监测得到了提高。在这里,我们总结了最近取得的显著进展和紧迫挑战,如 PD-(L)1 耐药性 MCC 以及免疫功能障碍 MCC 患者的管理。我们还强调了各种资源,以便提供者能够利用该领域的最新进展。