Department of Neurology, University of Heidelberg, Heidelberg, Germany; Department of Neurology, University of Halle-Wittenberg, Halle-Saale, Germany.
Department of Medicine V, Hematology, Oncology and Rheumatology, University of Heidelberg, Heidelberg, Germany.
ESMO Open. 2021 Dec;6(6):100317. doi: 10.1016/j.esmoop.2021.100317. Epub 2021 Nov 25.
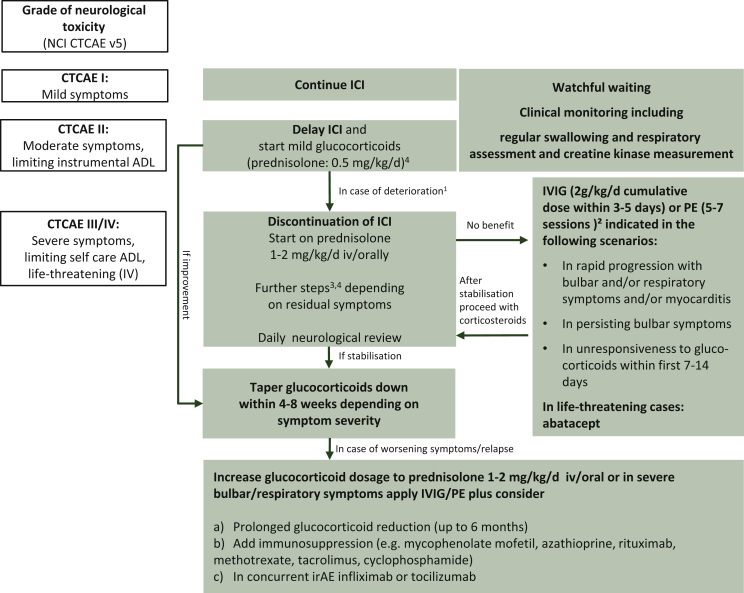
Immune-related neuromuscular adverse events are rare, but potentially life-threatening side-effects of immune checkpoint inhibitors (ICIs). They usually arise within the first 3 months after initiation of ICIs. Subacute symptom onset with more rapid progression than in idiopathic autoimmune neuromuscular diseases is typical. Prompt clinical diagnosis and treatment is essential for a favourable outcome. The importance of careful medical history and a well-established clinical diagnosis is emphasised rather than antibody detection or radiologic visualisation. Muscle weakness as a leading symptom can give rise to the suspicion of either neuropathy or myositis-myasthenia complex and differentiation may be complicated by their overlap. It is of utmost importance to recognise immune-related myositis and monitor for myocardial as well as bulbar involvement that may rapidly lead to cardiac or respiratory failure, persisting disability or even a fatal outcome. Symptoms typically improve with ICI discontinuation and early administration of glucocorticoids (prednisolone 1-2 mg/kg/day) in patients markedly affected. Severe and persisting symptoms including myocardial or bulbar affection can require therapy escalation to steroid-sparing agents. In patients with mild symptoms, not influencing functional abilities, careful clinical monitoring while staying on ICI therapy may be sufficient. Re-challenging with ICIs may be considered in selected cases, based on the initial severity of immune-related adverse events (irAEs) and clinical disease course. Depending on the individual irAE characteristics, the decision should be preferably discussed in an interdisciplinary irAE expert team with an experienced neurologist, rheumatologist and/or cardiologist and take the patient's preferences into account. The yet unmet need of systematic data on treatment, follow-up results and options of re-challenge of ICI treatment in neuromuscular toxicity has to be particularly considered in the shared decision-making process.
免疫相关神经肌肉不良事件较为罕见,但却是免疫检查点抑制剂(ICI)的潜在致命副作用。这些不良事件通常在开始使用 ICI 后 3 个月内出现。其典型特征为亚急性起病,且症状进展较特发性自身免疫性神经肌肉疾病更快。及时进行临床诊断和治疗对获得良好预后至关重要。相较于抗体检测或影像学可视化,本文更强调仔细的病史和明确的临床诊断的重要性。以肌无力为主要表现的症状可能会引起对神经病变或肌炎-重症肌无力综合征的怀疑,其鉴别可能因两者的重叠而变得复杂。认识到免疫相关肌炎并监测可能迅速导致心脏或呼吸衰竭、持续残疾甚至致命结局的心肌和延髓受累至关重要。在受影响较大的患者中,停止使用 ICI 并早期给予糖皮质激素(泼尼松龙 1-2mg/kg/天)可使症状改善。包括心肌或延髓受累在内的严重和持续症状可能需要升级治疗方案,使用类固醇保留剂。对于症状轻微、不影响功能能力的患者,在继续 ICI 治疗的同时进行仔细的临床监测可能就足够了。在某些情况下,可根据初始免疫相关不良事件(irAE)的严重程度和临床疾病进程,重新考虑使用 ICI。根据个体 irAE 的特征,最好在具有丰富经验的神经科医生、风湿病学家和/或心脏病专家组成的跨学科 irAE 专家组中进行讨论,并考虑患者的意愿。在共同决策过程中,还必须特别考虑到神经肌肉毒性的治疗、随访结果和重新挑战 ICI 治疗方案的系统数据方面的尚未满足的需求。