Department of Oncology, Oslo University Hospital, Oslo, Norway.
Department of Cancer Genetics, Institute for Cancer Research, Oslo University Hospital, Oslo, Norway.
Cancer Epidemiol Biomarkers Prev. 2022 Feb;31(2):342-351. doi: 10.1158/1055-9965.EPI-21-0555. Epub 2021 Dec 1.
Patients with right-sided colon cancer (RCC) and left-sided colon cancer (LCC) differ clinically and molecularly. The main objective was to investigate stage-stratified survival and recurrence of RCC and LCC across four 10-year periods.
Patients diagnosed from 1977 to 2016 with colon adenocarcinoma were included from the Cancer Registry of Norway. Primary tumor location (PTL) was defined as RCC if proximal and LCC if distal to the splenic flexure. Multivariable regressions were used to estimate HRs for overall survival (OS), recurrence-free survival (RFS), survival after recurrence (SAR), and excess HRs (eHR) for relative survival (RS).
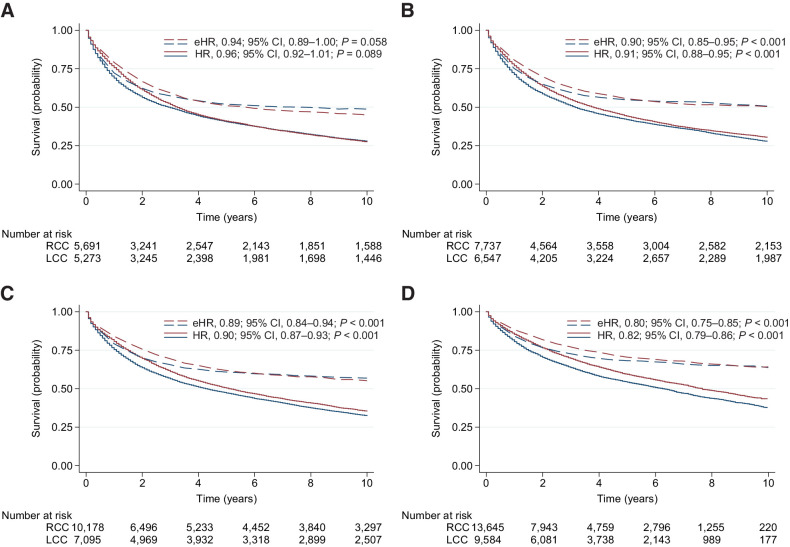
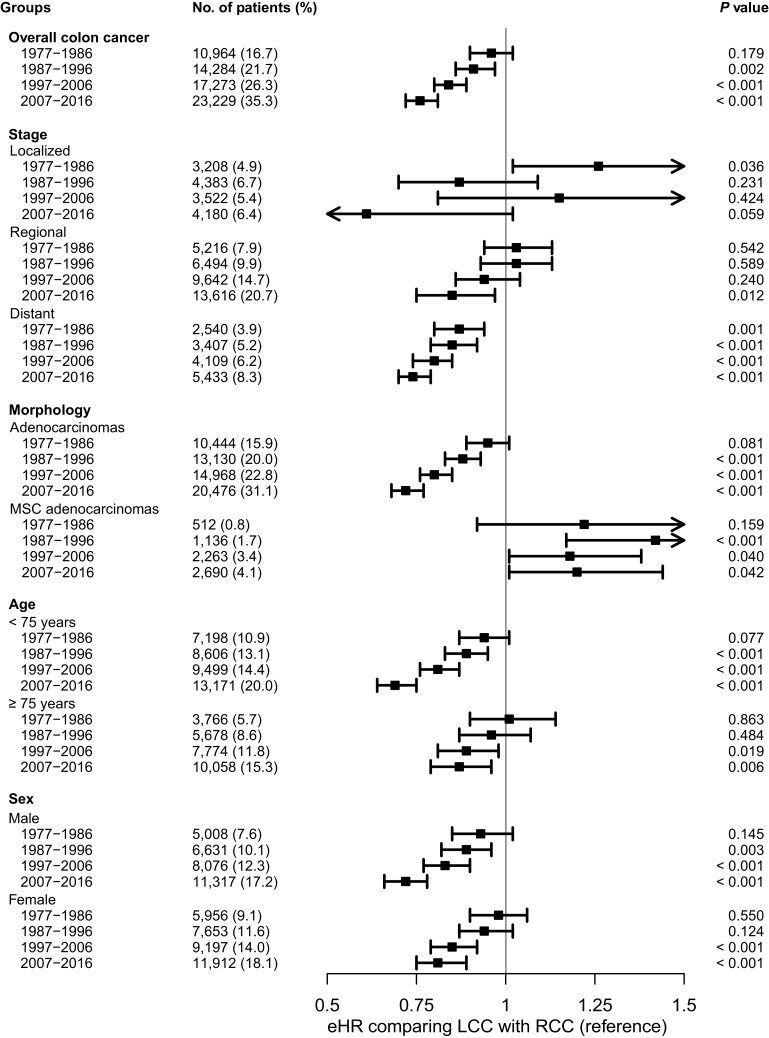
72,224 patients were eligible for analyses [55.1% ( = 39,769/72,224) had RCC]. In 1977 to 1986, there was no difference between LCC and RCC in OS [HR, 1.01; 95% confidence interval (CI), 0.97-1.06; = 0.581] or RS (eHR, 0.96; 95% CI, 0.90-1.02; = 0.179). In 2007 to 2016, LCC had significantly better OS (HR, 0.84; 95% CI, 0.80-0.87; < 0.001) and RS (eHR, 0.76; 95% CI, 0.72-0.81; < 0.001) compared with RCC. The gradually diverging and significantly favorable prognosis for LCC was evident for distant disease across all time periods and for regional disease from 2007 onward. There was no difference in RFS between LCC and RCC in patients less than 75 years during 2007 to 2016 (HR, 0.99; 95% CI, 0.91-1.08; = 0.819); however, SAR was significantly better for LCC (HR, 0.61; 95% CI, 0.53-0.71; < 0.001).
A gradually diverging and increasingly favorable prognosis was observed for patients with LCC with advanced disease over the past four decades.
Current PTL survival disparities stress the need for further exploring targetable molecular subgroups across and within different PTLs to further improve patient outcomes.
右侧结肠癌(RCC)和左侧结肠癌(LCC)患者在临床和分子水平上存在差异。主要目的是研究四个十年期间 RCC 和 LCC 的分层生存和复发情况。
从挪威癌症登记处纳入了 1977 年至 2016 年期间诊断为结肠腺癌的患者。如果肿瘤位于脾曲近端,则定义为 RCC,如果肿瘤位于脾曲远端,则定义为 LCC。多变量回归用于估计总生存(OS)、无复发生存(RFS)、复发后生存(SAR)和相对生存(RS)的超额 HR(eHR)。
共有 72224 名患者符合分析条件[55.1%(=39769/72224)为 RCC]。在 1977 年至 1986 年期间,LCC 和 RCC 的 OS(HR,1.01;95%置信区间[CI],0.97-1.06;=0.581)或 RS(eHR,0.96;95%CI,0.90-1.02;=0.179)没有差异。在 2007 年至 2016 年期间,LCC 的 OS(HR,0.84;95%CI,0.80-0.87;<0.001)和 RS(eHR,0.76;95%CI,0.72-0.81;<0.001)明显优于 RCC。在所有时间段,LCC 的远处疾病和从 2007 年开始的局部疾病的预后逐渐改善且明显优于 RCC。在 2007 年至 2016 年期间,75 岁以下患者的 RFS 无差异(HR,0.99;95%CI,0.91-1.08;=0.819);然而,LCC 的 SAR 明显更好(HR,0.61;95%CI,0.53-0.71;<0.001)。
在过去的四十年中,患有晚期疾病的 LCC 患者的预后逐渐改善,且预后越来越好。
目前 PTL 生存差异强调需要进一步探索不同 PTL 之间和内部的可靶向分子亚群,以进一步改善患者的预后。