D'Amore Jason, Meigher Stephen, Patterson Elizabeth, Sanapala Sowmya, Tarr Michael, Leisman Dan, Jones Michael, Moskovitz Joshua B, Offenbacher Joseph, Sperling Jeremy
Department of Emergency Medicine at the Jacobi Medical Center Albert Einstein College of Medicine Bronx New York USA.
Department of Emergency Medicine at the Jacobi and Montefiore Medical Centers Albert Einstein College of Medicine Bronx New York USA.
J Am Coll Emerg Physicians Open. 2021 Nov 24;2(6):e12563. doi: 10.1002/emp2.12563. eCollection 2021 Dec.
The goal of this study was to describe outcomes and associated characteristics of patients who were intubated during the initial (3/2020-4/2020) New York City surge of the severe acute respiratory syndrome coronavirus 2 (COVID-19) pandemic, during which time we were confronted by an unknown and unprecedented respiratory distress syndrome with extremely high degrees of morbidity and mortality. Our secondary aim was to analyze our physician's rapidly evolving approaches to COVID-19 airway management.
A retrospective cohort analysis of all patients intubated at two emergency departments (EDs) for COVID-19 suspected respiratory failure. In addition, a survey was done to analyze clinician airway management trends and attitudes as they evolved during that period.
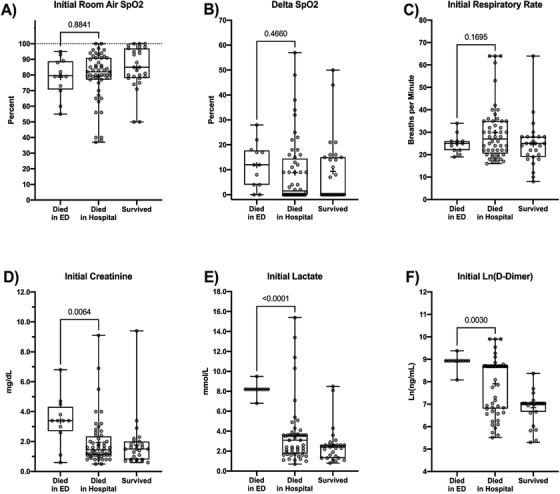
Ninety-five patients met inclusion criteria for the study. Primary outcomes looked at the spectrum of mortality outcomes ranging from died on arrival (DOA) to the ED, died in the ED (DED), died an inpatient (DIH), and survival to discharge. Overall mortalitywas 71.6% with an average age of 62.7 years. Female sex, as a demographic, was associated with higher rates of survival to discharge at 42.3% when compared to males at 23.2% ( < 0.001). Mean age was 70.8 years DOA, 65.6 years DED, 62.9 years DIH, and 60.0 years for survivors ( = 0.0037). Initial lactate levels were 8.15 mmol/L DED, 3.56 mmol/L DIH, and 2.61 mmol/L survivors ( < 0.0001). Initial creatinine levels were 3.38 mg/dL DED, 1.94 mg/dL DIH, and 1.77 mg/dL survivors ( = 0.0073). D-dimer levels were 7520.5 ng/mL DED, 5932.4 ng/mL DIH, and 1133.9 ng/mL survivors ( = 0.0045). Physician survey respondents reported high levels (69%) of laryngeal edema and prolonged post intubation hypoxia (>50% of time) and >80% remained concerned for their safety. There was a dramatic shift from early (73% of time) to late intubation strategies (67% of time) or non-invasive approaches (28% of time) as the first surge of the pandemic evolved.
Our findings demonstrate that several demographic, clinical and laboratory parameters correlated with mortality in our cohort of patients intubated during the initial phase of the COVID-19 pandemic. These included male sex, advanced age, high levels of initial lactic acidosis, elevated D-dimer, and chronic kidney disease/acute kidney injury. In contrast, presenting respiratory characteristics were not correlated with mortality. In addition, our findings demonstrate that physician attitudes and strategies related to COVID-19 airway management evolved significantly and rapidly over the initial phase of the pandemic.
本研究的目的是描述在严重急性呼吸综合征冠状病毒2(COVID-19)大流行初期(2020年3月至2020年4月)纽约市疫情激增期间接受插管治疗的患者的结局及相关特征,在此期间,我们面临一种未知且前所未有的呼吸窘迫综合征,其发病率和死亡率极高。我们的次要目的是分析我们的医生对COVID-19气道管理的快速演变方法。
对在两个急诊科因疑似COVID-19呼吸衰竭而插管的所有患者进行回顾性队列分析。此外,还进行了一项调查,以分析在此期间临床医生气道管理趋势及态度的演变情况。
95名患者符合该研究的纳入标准。主要结局观察了从到达急诊科即死亡(DOA)、在急诊科死亡(DED)、住院期间死亡(DIH)到出院存活的一系列死亡结局。总体死亡率为71.6%,平均年龄为62.7岁。作为人口统计学特征,女性出院存活率较高,为42.3%,而男性为23.2%(P<0.001)。DOA患者的平均年龄为70.8岁,DED患者为65.6岁,DIH患者为62.9岁,存活患者为60.0岁(P=0.0037)。初始乳酸水平在DED患者中为8.15 mmol/L,DIH患者中为3.56 mmol/L,存活患者中为2.61 mmol/L(P<0.0001)。初始肌酐水平在DED患者中为3.38 mg/dL,DIH患者中为1.94 mg/dL,存活患者中为1.77 mg/dL(P=0.0073)。D-二聚体水平在DED患者中为7520.5 ng/mL,DIH患者中为5932.4 ng/mL,存活患者中为1133.9 ng/mL(P=0.0045)。参与调查的医生报告称,喉部水肿发生率较高(69%),插管后缺氧持续时间较长(>50%的时间),且>80%的医生仍担心自身安全。随着大流行的首次激增演变,从早期(73%的时间)到晚期插管策略(67%的时间)或无创方法(28%的时间)出现了显著转变。
我们的研究结果表明,在COVID-19大流行初期接受插管治疗的患者队列中,一些人口统计学、临床和实验室参数与死亡率相关。这些参数包括男性、高龄、高水平的初始乳酸酸中毒、D-二聚体升高以及慢性肾脏病/急性肾损伤。相比之下,呈现的呼吸特征与死亡率无关。此外,我们的研究结果表明,在大流行的初始阶段,医生与COVID-19气道管理相关的态度和策略发生了显著且快速的演变。