Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark.
Hospital Pharmacy Fyn, Odense University Hospital, Odense, Denmark.
JAMA Netw Open. 2021 Dec 1;4(12):e2136802. doi: 10.1001/jamanetworkopen.2021.36802.
Statin use is common in older persons. Given uncertainties in ongoing benefit, changes in health status, and shifting goals of care and preferences, statin discontinuation may be considered in some older persons, although there is currently little evidence to guide this decision.
To evaluate the association between statin discontinuation and the rate of major adverse cardiovascular events (MACE) among people aged 75 years or older who receive long-term statin treatment.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included all persons in Denmark aged 75 years or older who were treated with statins for at least 5 consecutive years as of January 1, 2011. Participants were followed up until December 31, 2016. Data were analyzed from July to November, 2020.
Statin discontinuation.
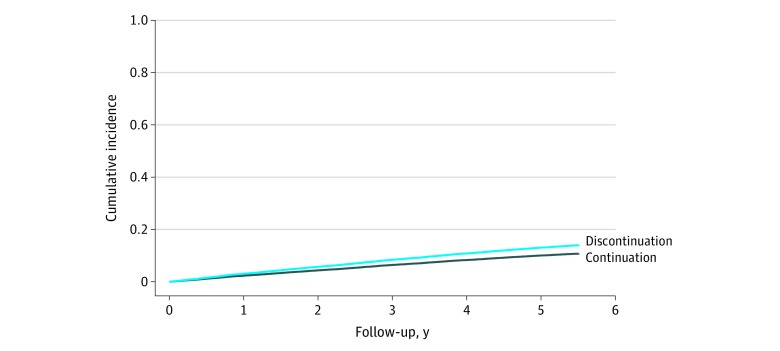
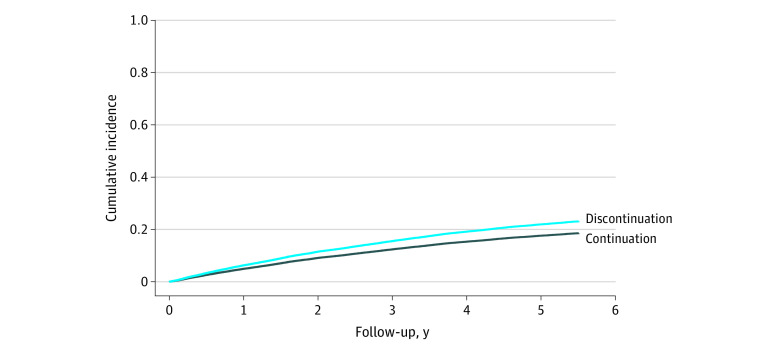
Rate of occurrence of MACE and its components (myocardial infarction, ischemic stroke or transient ischemic attack, coronary revascularization, and death due to myocardial infarction or ischemic stroke) in persons continuing statins compared with those discontinuing statins. Confounding adjustment was done using inverse probability of treatment weighting. Analyses were conducted separately for primary prevention (no history of cardiovascular disease) and secondary prevention (history of cardiovascular disease).
The study included 67 418 long-term statin users, including 27 463 in the primary prevention analysis (median age, 79 years [IQR, 77-83 years]; 18 134 [66%] female) and 39 955 in the secondary prevention analysis (median age, 80 years [IQR, 77-84 years]; 18 717 [47%] female). In both primary and secondary prevention analyses, the rate of MACE was higher among persons who discontinued statins compared with those who continued statins. In the primary prevention cohort, the weighted rate difference was 9 per 1000 person-years (95% CI, 5-12 per 1000 person-years) and the adjusted sub-hazard ratio was 1.32 (95% CI, 1.18-1.48), corresponding to 1 excess MACE per 112 persons who discontinued statins per year. In the secondary prevention cohort, the weighted rate difference was 13 per 1000 person-years (95% CI, 8-17 per 1000 person-years) and the adjusted sub-hazard ratio was 1.28 (95% CI, 1.18-1.39), corresponding to 1 excess MACE per 77 persons who discontinued statins per year.
In this cohort study, among older adults receiving long-term statin treatment, discontinuation of statins was associated with a higher rate of MACE compared with statin continuation in both the primary and the secondary prevention cohorts. These findings suggest a need for robust evidence from randomized clinical trials.
在老年人中,他汀类药物的使用较为常见。鉴于持续获益存在不确定性、健康状况变化以及治疗目标和偏好的转变,一些老年人可能会考虑停止使用他汀类药物,尽管目前几乎没有证据可以指导这一决定。
评估在接受长期他汀类药物治疗的 75 岁及以上人群中,停止使用他汀类药物与主要不良心血管事件(MACE)发生率之间的关系。
设计、地点和参与者:本队列研究纳入了 2011 年 1 月 1 日起至少连续 5 年接受他汀类药物治疗的丹麦所有 75 岁及以上人群。参与者的随访时间截至 2016 年 12 月 31 日。数据分析时间为 2020 年 7 月至 11 月。
他汀类药物停药。
与继续使用他汀类药物的患者相比,停止使用他汀类药物的患者发生 MACE 及其组成部分(心肌梗死、缺血性卒中和短暂性脑缺血发作、冠状动脉血运重建以及心肌梗死或缺血性卒中等原因导致的死亡)的发生率。使用逆概率治疗加权法进行混杂调整。分别对一级预防(无心血管疾病史)和二级预防(有心血管疾病史)进行分析。
这项研究纳入了 67418 名长期使用他汀类药物的患者,其中一级预防分析中包括 27463 名患者(中位年龄为 79 岁[四分位距(IQR),77-83 岁];18134 名[66%]女性),二级预防分析中包括 39955 名患者(中位年龄为 80 岁[IQR,77-84 岁];18717 名[47%]女性)。在一级和二级预防分析中,停止使用他汀类药物的患者 MACE 发生率均高于继续使用他汀类药物的患者。在一级预防队列中,加权率差为 9/1000 人年(95%CI,5-12/1000 人年),调整后的亚危险比为 1.32(95%CI,1.18-1.48),这意味着每年有 112 名停止使用他汀类药物的患者会发生 1 例额外的 MACE。在二级预防队列中,加权率差为 13/1000 人年(95%CI,8-17/1000 人年),调整后的亚危险比为 1.28(95%CI,1.18-1.39),这意味着每年有 77 名停止使用他汀类药物的患者会发生 1 例额外的 MACE。
在这项队列研究中,在接受长期他汀类药物治疗的老年患者中,与继续使用他汀类药物相比,他汀类药物停药与主要心血管不良事件(MACE)发生率增加相关,无论在一级预防还是二级预防队列中均如此。这些发现表明需要来自随机临床试验的有力证据。