Gothenburg Paediatric Growth Research Centre (GP-GRC), The Institute of Clinical Sciences, The Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden.
Department of Physiology/Endocrinology, The Institute of Neurosciences and Physiology, The Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden.
Front Endocrinol (Lausanne). 2021 Nov 9;12:737893. doi: 10.3389/fendo.2021.737893. eCollection 2021.
Despite different genetic background, Noonan syndrome (NS) shares similar phenotype features to Turner syndrome (TS) such as short stature, webbed neck and congenital heart defects. TS is an entity with decreased growth hormone (GH) responsiveness. Whether this is found in NS is debated.
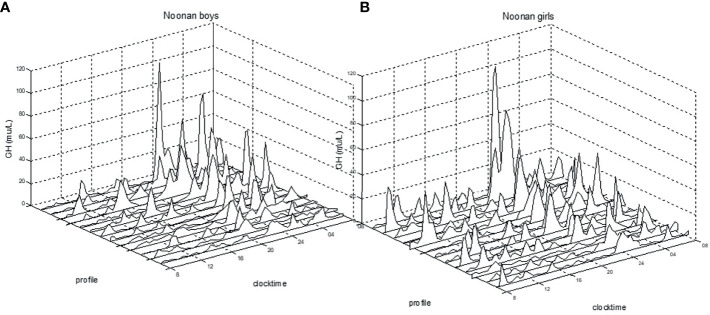
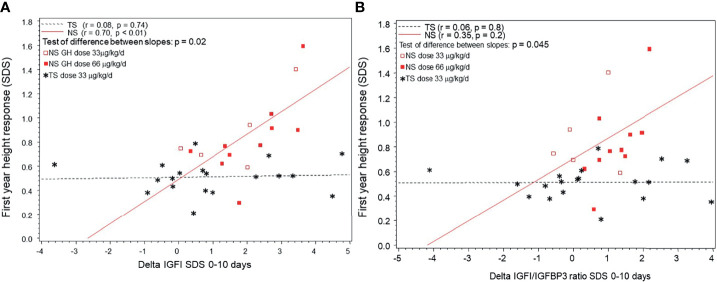
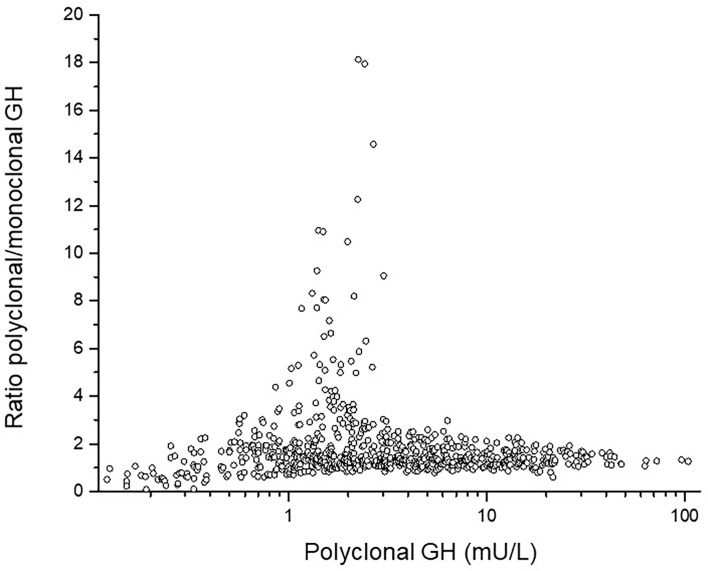
Data were retrieved from combined intervention studies including 25 children diagnosed with NS, 40 diagnosed with TS, and 45 control children (all prepubertal). NS-children and TS-girls were rhGH treated after investigation of the GH/IGFI-axis. GH was measured with poly- and monoclonal antibodies; 24hGH-profile pattern analysed by PULSAR. The NS-children were randomly assigned to Norditropin 33 or 66 μg/kg/day, and TS-girls were consecutively treated with Genotropin 33 or 66 μg/kg/day.
Higher PULSAR-estimates of 24h-profiles were found in both NS-children and TS-girls compared to controls: Polyclonal GH24h-profile (Mean ± SD) was higher in both groups (44 ± 23mU/L, p<0.01 in NS; 51 ± 47, p<0.001 in TS; compared to 30 ± 23 mU/L in controls) as was GH-baseline (1.4 ± 0.6 mU/L in NS; 2.4 ± 2.4 mU/L in TS, p<0.01 for both, compared to 1.1 ± 1.2 mU/L in controls). Pre-treatment IGFI was 2.2 lower in NS-children (-1.7 ± 1.3) compared to TS-girls (0.6 ± 1.8, p<0.0001). GH, IGFI/IGFBP3-ratio, and chronological age at start of GH accounted for 59% of the variance in first-year growth response in NS.
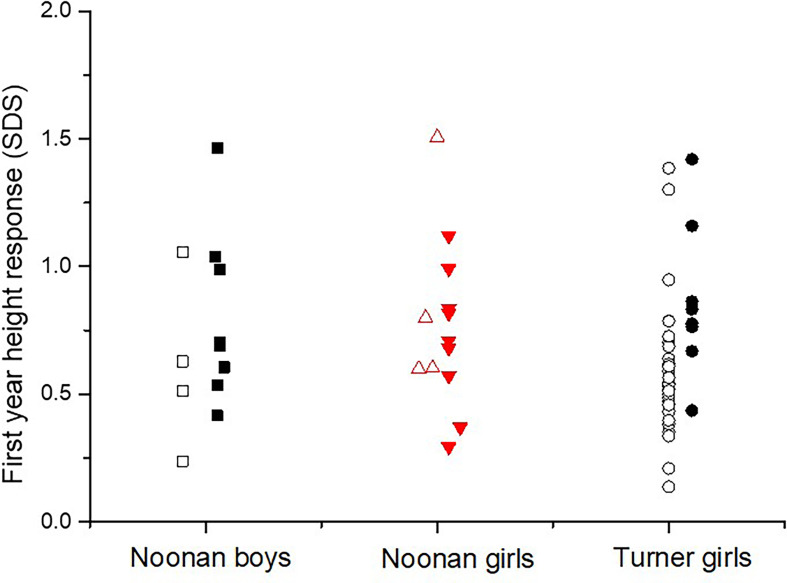
Both prepubertal NS-children and TS-girls had a high GH secretion, but low IGFI/IGFBP3 levels only in NS-children. Both groups presented a broad individual response. NS-children showed higher response in IGFI and growth, pointing to higher responsiveness to GH treatment than TS-girls.
尽管遗传背景不同,努南综合征(Noonan syndrome,NS)与特纳综合征(Turner syndrome,TS)具有相似的表型特征,如身材矮小、颈蹼和先天性心脏病。TS 是一种生长激素(growth hormone,GH)反应降低的实体。这种情况是否存在于 NS 中存在争议。
数据来自包括 25 名 NS 患儿、40 名 TS 患儿和 45 名对照儿童(均为青春期前)的联合干预研究中。在研究 GH/IGFI 轴后,对 NS 患儿和 TS 女孩进行了 GH 治疗。使用多克隆和单克隆抗体测量 GH;通过 PULSAR 分析 24 小时 GH 谱模式。NS 患儿被随机分配接受 Norditropin 33 或 66 μg/kg/天,TS 女孩连续接受 Genotropin 33 或 66 μg/kg/天治疗。
与对照组相比,NS 患儿和 TS 女孩的 PULSAR 24 小时谱估计值更高:两组多克隆 GH24 小时谱(均值±标准差)均较高(NS 组为 44±23mU/L,p<0.01;TS 组为 51±47,p<0.001;对照组为 30±23mU/L),GH 基线也较高(NS 组为 1.4±0.6mU/L;TS 组为 2.4±2.4mU/L,均 p<0.01,对照组为 1.1±1.2mU/L)。与 TS 女孩相比,NS 患儿的 IGFI 预治疗值低 2.2(-1.7±1.3)(p<0.0001)。GH、IGFI/IGFBP3 比值和 GH 治疗开始时的实际年龄占 NS 患儿第一年生长反应的 59%。
青春期前的 NS 患儿和 TS 女孩均有较高的 GH 分泌,但仅在 NS 患儿中 IGFI/IGFBP3 水平较低。两组均表现出广泛的个体反应。NS 患儿的 IGFI 和生长反应更高,表明对 GH 治疗的反应性高于 TS 女孩。