Sinha Arjun, Rivera Adovich S, Chadha Simran A, Prasada Sameer, Pawlowski Anna E, Thorp Edward, DeBerge Matthew, Ramsey-Goldman Rosalind, Lee Yvonne C, Achenbach Chad J, Lloyd-Jones Donald M, Feinstein Matthew J
Department of Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States.
Department of Preventive Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States.
Front Cardiovasc Med. 2021 Nov 10;8:757738. doi: 10.3389/fcvm.2021.757738. eCollection 2021.
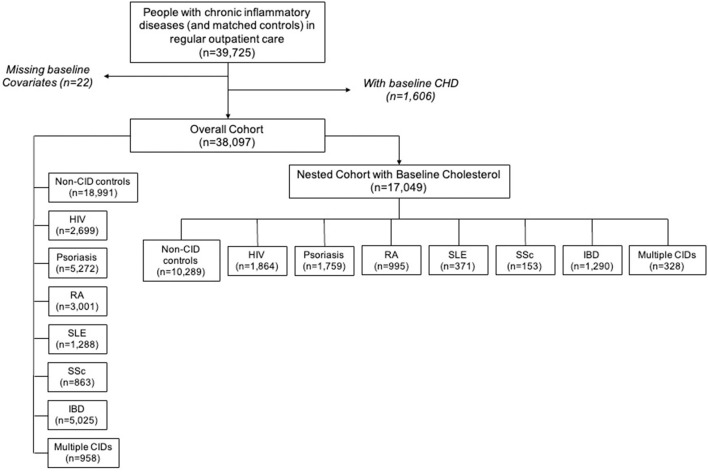
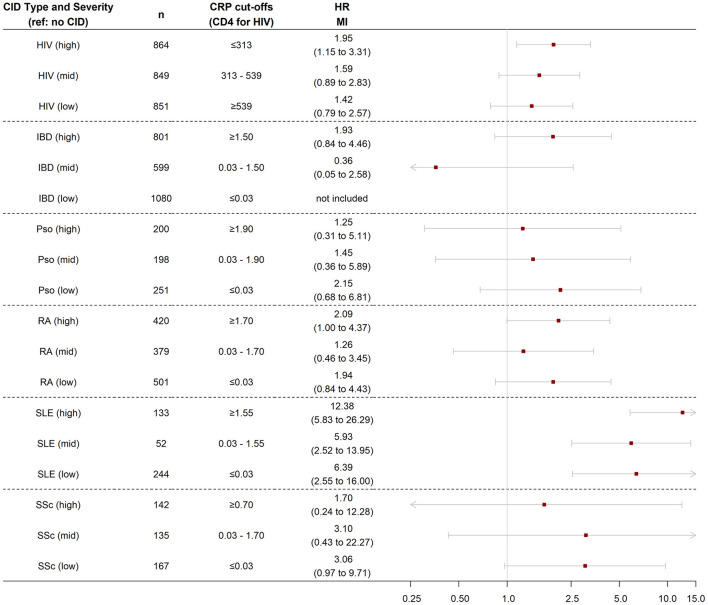
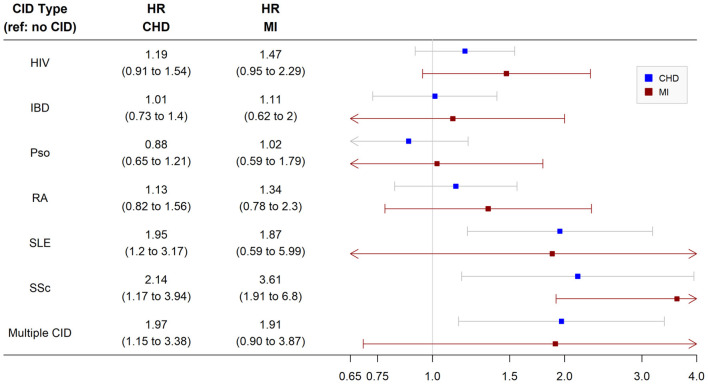
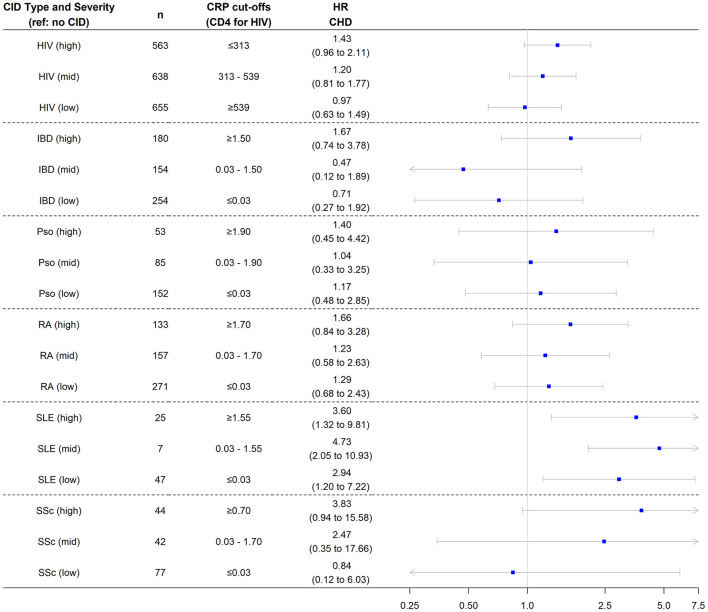
Chronic inflammatory diseases (CIDs) are considered risk enhancing factors for coronary heart disease (CHD). However, sparse data exist regarding relative CHD risks across CIDs. Determine relative differences in CHD risk across multiple CIDs: psoriasis, rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), human immunodeficiency virus (HIV), systemic sclerosis (SSc), and inflammatory bowel disease (IBD). The cohort included patients with CIDs and controls without CID in an urban medical system from 2000 to 2019. Patients with CIDs were frequency-matched with non-CID controls on demographics, hypertension, and diabetes. CHD was defined as myocardial infarction (MI), ischemic heart disease, and/or coronary revascularization based on validated administrative codes. Multivariable-adjusted Cox models were used to determine the risk of incident CHD and MI for each CID relative to non-CID controls. In secondary analyses, we compared CHD risk by disease severity within each CID. Of 17,049 patients included for analysis, 619 had incident CHD (202 MI) over an average of 4.4 years of follow-up. The multivariable-adjusted risk of CHD was significantly higher for SLE [hazard ratio (HR) 1.9, 95% confidence interval (CI) 1.2, 3.2] and SSc (HR 2.1, 95% CI 1.2, 3.9). Patients with SLE also had a significantly higher risk of MI (HR 3.6, 95% CI 1.9, 6.8). When CIDs were categorized by markers of disease severity (C-reactive protein for all CIDs except HIV, for which CD4 T cell count was used), greater disease severity was associated with higher CHD risk across CIDs. Patients with SLE and SSc have a higher risk of CHD. CHD risk with HIV, RA, psoriasis, and IBD may only be elevated in those with greater disease severity. Clinicians should personalize CHD risk and treatment based on type and severity of CID.
慢性炎症性疾病(CIDs)被认为是冠心病(CHD)的风险增强因素。然而,关于不同CIDs相对CHD风险的数据却很稀少。确定多种CIDs(银屑病、类风湿性关节炎(RA)、系统性红斑狼疮(SLE)、人类免疫缺陷病毒(HIV)、系统性硬化症(SSc)和炎症性肠病(IBD))之间CHD风险的相对差异。该队列包括2000年至2019年期间城市医疗系统中患有CIDs的患者和未患CIDs的对照。患有CIDs的患者在人口统计学、高血压和糖尿病方面与非CIDs对照进行频率匹配。CHD根据经过验证的行政代码定义为心肌梗死(MI)、缺血性心脏病和/或冠状动脉血运重建。使用多变量调整的Cox模型确定每种CIDs相对于非CIDs对照发生CHD和MI的风险。在二次分析中,我们比较了每种CIDs内疾病严重程度的CHD风险。在纳入分析的17049名患者中,平均4.4年的随访期间有619人发生CHD(202例MI)。SLE [风险比(HR)1.9,95%置信区间(CI)1.2,3.2]和SSc(HR 2.1,95%CI 1.2,3.9)的多变量调整CHD风险显著更高。SLE患者发生MI的风险也显著更高(HR 3.6,95%CI 1.9,6.8)。当根据疾病严重程度标志物对CIDs进行分类时(除HIV外所有CIDs使用C反应蛋白,HIV使用CD4 T细胞计数),在所有CIDs中,疾病严重程度越高,CHD风险越高。SLE和SSc患者患CHD的风险更高。HIV、RA、银屑病和IBD的CHD风险可能仅在疾病严重程度较高的患者中升高。临床医生应根据CIDs的类型和严重程度对CHD风险和治疗进行个性化。