Aghili Mina, Kasturirangan Meera Neelathahalli
Department of Pharmacy Practice, Visveswarapura Institute of Pharmaceutical Sciences, Rajiv Gandhi University of Health Sciences, Bengaluru, Karnataka, India; Department of Pharmacy Practice, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bengaluru, Karnataka, India.
Indian J Crit Care Med. 2021 Nov;25(11):1226-1231. doi: 10.5005/jp-journals-10071-23919.
Drug-drug interactions (DDIs) can create a burden on prescribers to preserve patient safety. This study aimed to identify common DDIs in critically ill patients with chronic kidney disease (CKD) and to evaluate clinical pharmacist's interventions in managing DDIs among these patients.
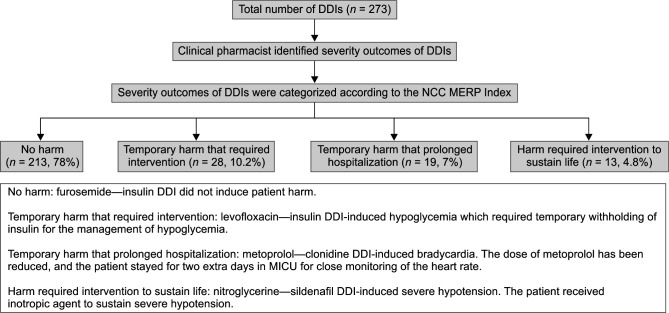
A prospective observational study was conducted from October 2018 to March 2019. The clinical pharmacist performed a medication chart review; DDIs were identified by using Lexicomp drug interaction. Based on the occurrence of DDIs, patients were divided into group A: patients with DDI ( = 76) and group B: patients without DDI ( = 15). Clinical pharmacist's interventions were classified according to Pharmaceutical Care Network Europe. The National Coordinating Council for Medication Error Reporting and Prevention was used to categorize the severity outcomes of DDIs and the degree of patient harm.
A total of 273 DDIs were identified. The majority of DDIs (63.7%) required close monitoring of the therapeutic outcome to ensure maintaining patient safety. DDIs that needed to be managed by considering therapy modification and avoiding drug combination were accounted for 17.2 and 12.8% of the most common detected interactions, respectively. Seventy-eight percent of DDIs induced no harm to patient. Clinical pharmacist provided different types of recommendations to manage detected interactions, which ranged from therapy outcome monitoring to stop DDIs. A great proportion of pharmacist's interventions (92%) were accepted by prescribers. Compared to patients with stage 3 and 4 CKD, patients with stage 5 had a significantly higher number of DDIs (stage 3 vs 5: = 0.0019, stage 4 vs 5: = 0.0456). The number of comorbidities ( = 0.0003) and ( <0.0001) medications were found to be significantly greater in group A.
Clinical pharmacist performed important interventions in timely identifying, managing DDIs, and prevention of associated patient harms.
Aghili M, Kasturirangan MN. Management of Drug-Drug Interactions among Critically Ill Patients with Chronic Kidney Disease: Impact of Clinical Pharmacist's Interventions. Indian J Crit Care Med 2021;25(11):1226-1231.
药物相互作用(DDIs)会给开处方者带来负担,以保障患者安全。本研究旨在确定慢性肾脏病(CKD)重症患者中常见的药物相互作用,并评估临床药师对这些患者药物相互作用管理的干预措施。
于2018年10月至2019年3月进行了一项前瞻性观察研究。临床药师对用药记录进行审查;使用Lexicomp药物相互作用软件识别药物相互作用。根据药物相互作用的发生情况,将患者分为A组:发生药物相互作用的患者(n = 76)和B组:未发生药物相互作用的患者(n = 15)。临床药师的干预措施根据欧洲药学保健网络进行分类。使用国家药物错误报告和预防协调委员会对药物相互作用的严重程度结果和对患者造成伤害的程度进行分类。
共识别出273例药物相互作用。大多数药物相互作用(63.7%)需要密切监测治疗结果以确保患者安全。需要通过考虑调整治疗方案和避免药物联用进行管理的药物相互作用分别占最常见检测到的相互作用的17.2%和12.8%。78%的药物相互作用未对患者造成伤害。临床药师针对检测到的相互作用提供了不同类型的建议,范围从监测治疗结果到停用药物相互作用。很大一部分药师的干预措施(92%)被开处方者接受。与3期和4期慢性肾脏病患者相比,5期患者的药物相互作用数量显著更高(3期与5期比较:P = 0.0019,4期与5期比较:P = 0.0456)。发现A组患者的合并症数量(P = 0.0003)和用药数量(P <0.0001)显著更多。
临床药师在及时识别、管理药物相互作用以及预防相关患者伤害方面发挥了重要干预作用。
Aghili M, Kasturirangan MN. 慢性肾脏病重症患者药物相互作用的管理:临床药师干预的影响。《印度重症医学杂志》2021;25(11):1226 - 1231。