Medical Research Centre, University of Waikato, Hamilton, New Zealand.
Auckland University of Technology, Auckland, New Zealand.
Fam Pract. 2022 Jul 19;39(4):639-647. doi: 10.1093/fampra/cmab155.
New Zealand (NZ) has high rates of colorectal cancer (CRC) but low rates of early detection. The majority of CRC is diagnosed through general practice, where lengthy diagnostic intervals are common. We investigated factors contributing to diagnostic delay in a cohort of patients newly diagnosed with CRC.
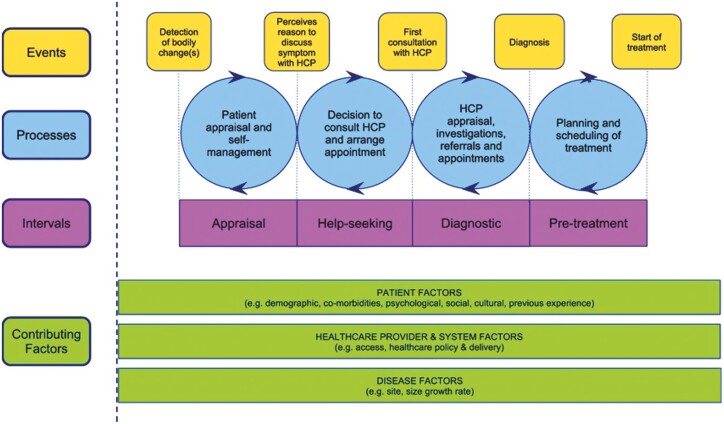
Patients were recruited from the Midland region and interviewed about their diagnostic experience using a questionnaire based on a modified Model of Pathways to Treatment framework and SYMPTOM questionnaire. Descriptive statistics were used to describe the population characteristics. Chi-square analysis and logistic regression were used to analyse factors influencing diagnostic intervals.
Data from 176 patients were analysed, of which 65 (36.9%) experienced a general practitioner (GP) diagnostic interval of >120 days and 96 (54.5%) experienced a total diagnostic interval (TDI) > 120 days. Patients reporting rectal bleeding were less likely to experience a long TDI (odds ratio [OR] 0.34, 95% confidence interval [CI]: 0.14-0.78) and appraisal/help-seeking interval (OR, 0.19, 95% CI: 0.06-0.59). Patients <60 were more likely to report a longer appraisal/help-seeking interval (OR, 3.32, 95% CI: 1.17-9.46). Female (OR, 2.19, 95% CI: 1.08-4.44) and Māori patients (OR, 3.18, 95% CI: 1.04-9.78) were more likely to experience a long GP diagnostic interval.
NZ patients with CRC can experience long diagnostic intervals, attributed to patient and health system factors. Young patients, Māori, females, and patients experiencing change of bowel habit may be at particular risk. We need to increase symptom awareness of CRC for patients and GPs. Concentrated efforts are needed to ensure equity for Māori in access to screening, diagnostics, and treatment.
新西兰(NZ)结直肠癌(CRC)发病率较高,但早期发现率较低。大多数 CRC 是通过全科医生诊断出来的,而在那里,诊断间隔通常很长。我们调查了新诊断为 CRC 的患者队列中导致诊断延迟的因素。
从米德兰地区招募患者,并使用基于改良治疗途径模型和症状问卷的问卷对其诊断经验进行访谈。使用描述性统计来描述人群特征。使用卡方分析和逻辑回归分析影响诊断间隔的因素。
对 176 名患者的数据进行了分析,其中 65 名(36.9%)的全科医生(GP)诊断间隔超过 120 天,96 名(54.5%)的总诊断间隔(TDI)超过 120 天。报告直肠出血的患者不太可能经历较长的 TDI(优势比[OR]0.34,95%置信区间[CI]:0.14-0.78)和评估/寻求帮助间隔(OR,0.19,95%CI:0.06-0.59)。<60 岁的患者更有可能报告较长的评估/寻求帮助间隔(OR,3.32,95%CI:1.17-9.46)。女性(OR,2.19,95%CI:1.08-4.44)和毛利人患者(OR,3.18,95%CI:1.04-9.78)更有可能经历较长的 GP 诊断间隔。
新西兰 CRC 患者可能会经历较长的诊断间隔,这归因于患者和卫生系统因素。年轻患者、毛利人、女性和经历排便习惯改变的患者可能面临特别高的风险。我们需要提高患者和全科医生对 CRC 症状的认识。需要集中精力确保毛利人在获得筛查、诊断和治疗方面的公平性。