Elegbede Anifat A, Gibson Amanda J, Fung Andrea S, Cheung Winson Y, Dean Michelle L, Bebb D Gwyn, Pabani Aliyah
Department of Oncology, University of Calgary, Calgary, Alberta, Canada.
Cancer Centre of Southeastern Ontario, Kingston Health Sciences Centre, Kingston, Ontario, Canada.
JTO Clin Res Rep. 2021 Oct 28;2(12):100249. doi: 10.1016/j.jtocrr.2021.100249. eCollection 2021 Dec.
The real-world data evaluating treatment outcomes of atezolizumab plus carboplatin-etoposide chemotherapy (atezolizumab) for extensive-stage SCLC (ESCLC) are lacking. Our objective was to evaluate real-world outcomes of ESCLC treated with atezolizumab.
A retrospective analysis of provincial patients with ESCLC who started first-line (1L) systemic treatment was conducted. We primarily evaluated the progression-free survival (PFS) and overall survival (OS) outcomes in association with atezolizumab compared with platinum-etoposide chemotherapy (chemotherapy) while adjusting for relevant demographic and clinical factors. Adverse events (AEs) during 1L were evaluated.
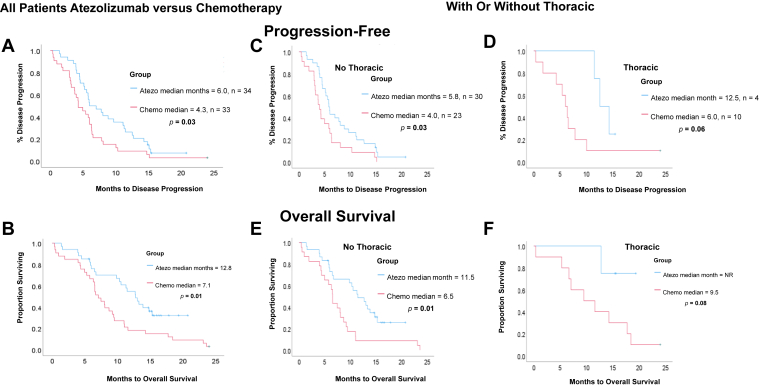
A total of 67 patients were identified. Of the 34 patients who received atezolizumab, 24% had Eastern Cooperative Oncology Group performance status greater than or equal to 2, approximately 50% were more than or equal to 65 years, 21% received cisplatin-etoposide chemotherapy before atezolizumab, and 12% had thoracic radiation (tRT).Within the atezolizumab versus chemotherapy group, the median PFS equals to 6.0 versus 4.3 months ( = 0.03) whereas OS = 12.8 versus 7.1 months ( = 0.01). Relative to chemotherapy, the hazard ratio (95% confidence interval) for PFS was 0.53 (0.28-1.02) and OS was 0.42 (0.20-0.88) with atezolizumab. tRT compared with no tRT receipt correlated with reduced death risk (hazard ratio [95% confidence interval] = 0.33 [0.13-0.88]).AE-related treatment withdrawal with atezolizumab was 32% and 15% with chemotherapy ( = 0.02). Within the tRT subgroup, 25% versus 20% in atezolizumab versus chemotherapy group, respectively, discontinued 1L owing to AE.
This is the first real-world study revealing comparable survival with that in the IMpower133 trial. Treatment discontinuation from AEs was higher with atezolizumab among Canadian patients with ESCLC. Our data suggest safe use of tRT and chemoimmunotherapy, but its efficacy for ESCLC warrants further study.
缺乏评估阿替利珠单抗联合卡铂-依托泊苷化疗(阿替利珠单抗)治疗广泛期小细胞肺癌(ESCLC)治疗效果的真实世界数据。我们的目的是评估接受阿替利珠单抗治疗的ESCLC的真实世界疗效。
对开始一线(1L)全身治疗的省级ESCLC患者进行回顾性分析。我们主要评估了与铂类-依托泊苷化疗(化疗)相比,阿替利珠单抗治疗的无进展生存期(PFS)和总生存期(OS)结果,同时对相关人口统计学和临床因素进行了调整。评估了1L治疗期间的不良事件(AE)。
共纳入67例患者。在接受阿替利珠单抗治疗的34例患者中,24%的东部肿瘤协作组体能状态大于或等于2,约50%的患者年龄大于或等于65岁,21%的患者在接受阿替利珠单抗治疗前接受过顺铂-依托泊苷化疗,12%的患者接受过胸部放疗(tRT)。在阿替利珠单抗组与化疗组中,中位PFS分别为6.0个月和4.3个月(P = 0.03),而OS分别为12.8个月和7.1个月(P = 0.01)。与化疗相比,阿替利珠单抗治疗的PFS风险比(95%置信区间)为0.53(0.28 - 1.02),OS风险比为0.42(0.20 - 0.88)。与未接受tRT相比,接受tRT与死亡风险降低相关(风险比[95%置信区间]= 0.33[0.13 - 0.88])。阿替利珠单抗因AE导致的治疗中断率为32%,化疗为15%(P = 0.02)。在tRT亚组中,阿替利珠单抗组和化疗组分别有25%和20%的患者因AE中断1L治疗。
这是第一项揭示与IMpower133试验相当生存期的真实世界研究。在加拿大ESCLC患者中,阿替利珠单抗因AE导致的治疗中断率更高。我们的数据表明tRT和化疗免疫疗法的使用是安全的,但其对ESCLC的疗效值得进一步研究。