Department of Laboratory Medicine, Yale University School of Medicine, New Haven, CT.
Department of Pediatrics, Yale University School of Medicine, New Haven, CT.
Hematology Am Soc Hematol Educ Program. 2021 Dec 10;2021(1):704-709. doi: 10.1182/hematology.2021000308.
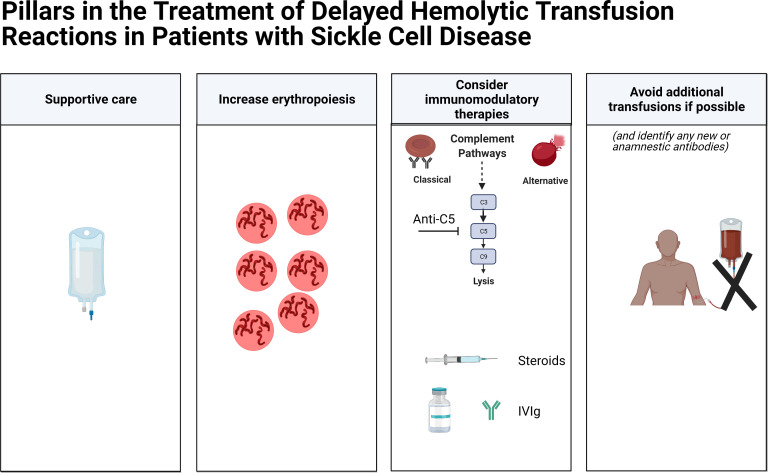
Delayed hemolytic transfusion reactions (DHTRs) in patients with sickle cell disease are underappreciated and potentially fatal. Patients with DHTRs typically have symptoms of pain or dark urine days to weeks following a red blood cell (RBC) transfusion. In instances of DHTRs with hyperhemolysis, the patient's hemoglobin (Hgb) may be significantly lower than it was pretransfusion, and the Hgb A may drop by more than 50%. In most cases, at least 1 RBC alloantibody and sometimes multiple RBC alloantibodies can be identified during the DHTR, with those antibodies presumably having fallen below the level of detection at the time of the implicated transfusion. However, in up to one-third of cases, no new RBC alloantibodies can be identified posttransfusion. Complement is increasingly being appreciated to play a role in DHTRs and hyperhemolysis, not only due to classic pathway activation (with complement fixed antibody bound to RBCs) but also due to alternative pathway activation (resulting in part from plasma free heme). As such, anti-C5 inhibition has recently been reported to be effective at mitigating hemolysis in the setting of some severe DHTRs. Transfusion avoidance during DHTRs is recommended if possible, with long-term transfusion support advice being less clear; for example, a history of a severe DHTR may lead to questions regarding the safety of transfusions prior to curative therapies such as stem cell transplantation or gene therapy. A better understanding of antibody-positive and antibody-negative DHTRs, including patient- or disease-specific risk factors, is necessary to improve transfusion safety.
镰状细胞病患者的迟发性溶血性输血反应(DHTR)未被充分认识,且可能致命。DHTR 患者通常在输血后数天至数周出现疼痛或深色尿液等症状。在伴有严重溶血的 DHTR 中,患者的血红蛋白(Hgb)可能明显低于输血前水平,Hgb A 可能下降超过 50%。在大多数情况下,至少可以在 DHTR 期间鉴定出 1 种 RBC 同种抗体,有时甚至可以鉴定出多种 RBC 同种抗体,这些抗体在发生相关输血时可能已低于检测水平。然而,高达三分之一的病例在输血后无法鉴定出新的 RBC 同种抗体。越来越多的证据表明补体在 DHTR 和严重溶血中发挥作用,不仅是由于经典途径的激活(补体固定抗体与 RBC 结合),还由于替代途径的激活(部分是由于血浆游离血红素)。因此,最近有报道称,抗 C5 抑制在某些严重 DHTR 中可有效减轻溶血。如果可能,建议在 DHTR 期间避免输血,而长期输血支持的建议则不太明确;例如,严重 DHTR 的病史可能会导致在进行根治性治疗(如干细胞移植或基因治疗)之前对输血安全性产生疑问。需要更好地了解抗体阳性和抗体阴性的 DHTR,包括患者或疾病特异性的危险因素,以提高输血安全性。