Department of Global Health, University of Washington, Seattle, Washington, USA.
Centre for Microbiology Research, Kenya Medical Research Institute, Nairobi, Kenya.
J Int AIDS Soc. 2021 Dec;24(12):e25845. doi: 10.1002/jia2.25845.
In public clinics in Kenya, separate, sequential delivery of the component services of pre-exposure prophylaxis (PrEP) (e.g. HIV testing, counselling, and dispensing) creates long wait times that hinder clients' ability and desire to access and continue PrEP. We conducted a mixed methods study in four public clinics in western Kenya to identify strategies for operationalizing a one-stop shop (OSS) model and evaluate whether this model could improve client wait time and care acceptability among clients and providers without negatively impacting uptake or continuation.
From January 2020 through November 2020, we collected and analysed 47 time-and-motion observations using Mann-Whitney U tests, 29 provider and client interviews, 68 technical assistance reports, and clinic flow maps from intervention clinics. We used controlled interrupted time series (cITS) to compare trends in PrEP initiation and on-time returns from a 12-month pre-intervention period (January-December 2019) to an 8-month post-period (January-November 2020, excluding a 3-month COVID-19 wash-out period) at intervention and control clinics.
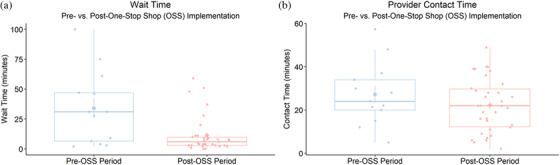
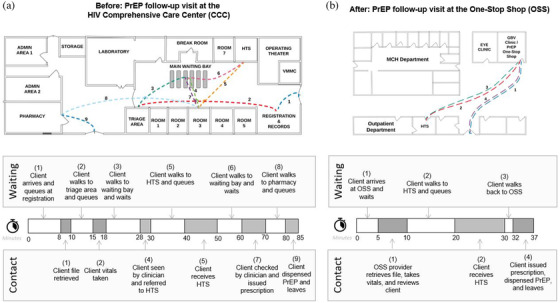
From the pre- to post-period, median client wait time at intervention clinics dropped significantly from 31 to 6 minutes (p = 0.02), while median provider contact time remained around 23 minutes (p = 0.4). Intervention clinics achieved efficiency gains by moving PrEP delivery to lower volume departments, moving steps closer together (e.g. relocating supplies; cross-training and task-shifting), and differentiating clients based on the subset of services needed. Clients and providers found the OSS model highly acceptable and additionally identified increased privacy, reduced stigma, and higher quality client-provider interactions as benefits of the model. From the pre- to post-period, average monthly initiations at intervention and control clinics increased by 6 and 2.3, respectively, and percent of expected follow-up visits occurring on time decreased by 18% and 26%, respectively; cITS analysis of PrEP initiations (n = 1227) and follow-up visits (n = 2696) revealed no significant difference between intervention and control clinics in terms of trends in PrEP initiation and on-time returns (all p>0.05).
An OSS model significantly improved client wait time and care acceptability without negatively impacting initiations or continuations, thus highlighting opportunities to improve the efficiency of PrEP delivery efficiency and client-centredness.
在肯尼亚的公立诊所,艾滋病毒前暴露预防(PrEP)的各个组成部分服务(如 HIV 检测、咨询和配药)分开、连续提供,导致患者的等待时间延长,从而阻碍了患者获得和继续 PrEP 的能力和意愿。我们在肯尼亚西部的四家公立诊所进行了一项混合方法研究,以确定实施一站式服务(OSS)模式的策略,并评估该模式是否可以改善患者的等待时间,并提高患者和提供者对 PrEP 的接受程度,而不会对 PrEP 的采用或持续产生负面影响。
从 2020 年 1 月到 11 月,我们在干预诊所收集并分析了 47 次工时观察数据,进行了 29 次提供者和患者访谈,68 次技术援助报告,并绘制了诊所流程图。我们使用控制中断时间序列(cITS)比较了在干预诊所和对照诊所中,从 2019 年 12 月的 12 个月前干预期到 2020 年 11 月的 8 个月后干预期(不包括 3 个月的 COVID-19 清洗期)期间 PrEP 启动和按时返回的趋势。
从干预前到干预后,干预诊所的患者平均等待时间从 31 分钟显著下降到 6 分钟(p = 0.02),而提供者的平均接触时间仍保持在 23 分钟左右(p = 0.4)。干预诊所通过将 PrEP 服务转移到低容量部门、将步骤靠近(例如重新布置用品;交叉培训和任务转移)以及根据所需服务的子集对患者进行区分,实现了效率的提高。患者和提供者发现 OSS 模型非常可接受,并且还发现增加隐私、减少污名化和提高患者-提供者互动的质量是该模型的好处。从干预前到干预后,干预诊所和对照诊所每月平均启动人数分别增加了 6 人和 2.3 人,按时进行的预期随访人数分别减少了 18%和 26%;对 1227 名 PrEP 启动者和 2696 名按时随访者进行的 cITS 分析显示,干预诊所和对照诊所的 PrEP 启动和按时随访趋势均无显著差异(均 p>0.05)。
OSS 模型显著缩短了患者的等待时间,提高了患者对护理的接受程度,同时没有对启动或持续产生负面影响,因此突显了提高 PrEP 服务效率和以患者为中心的机会。