Department of Oncology, Sun Yat-sen University Cancer Center, Guangzhou, China.
Department of Radiology, Zhejiang Cancer Hospital, Hangzhou, China.
J Immunother Cancer. 2021 Dec;9(12). doi: 10.1136/jitc-2021-003790.
This study aimed to evaluate the antitumor activity of camrelizumab, an antiprogrammed cell death-1 antibody, in pretreated recurrent or metastatic nasopharyngeal carcinoma (NPC) and to explore predictive biomarkers.
Patients with recurrent (not amenable to locally curative treatment) or metastatic NPC who had failed at least two lines of chemotherapy were eligible to receive camrelizumab (200 mg intravenously every 2 weeks) for 2 years or until disease progression, intolerable adverse events, withdrawal of consents, or investigator decision. The primary endpoint was objective response rate (ORR) assessed by an independent review committee (IRC). Programmed cell death-ligand 1 (PD-L1) expression was assessed by immunohistochemistry. Other immune-related biomarkers including major histocompatibility complex class I and major histocompatibility complex class II (MHC-II) were assessed by multiplex immunofluorescence staining.
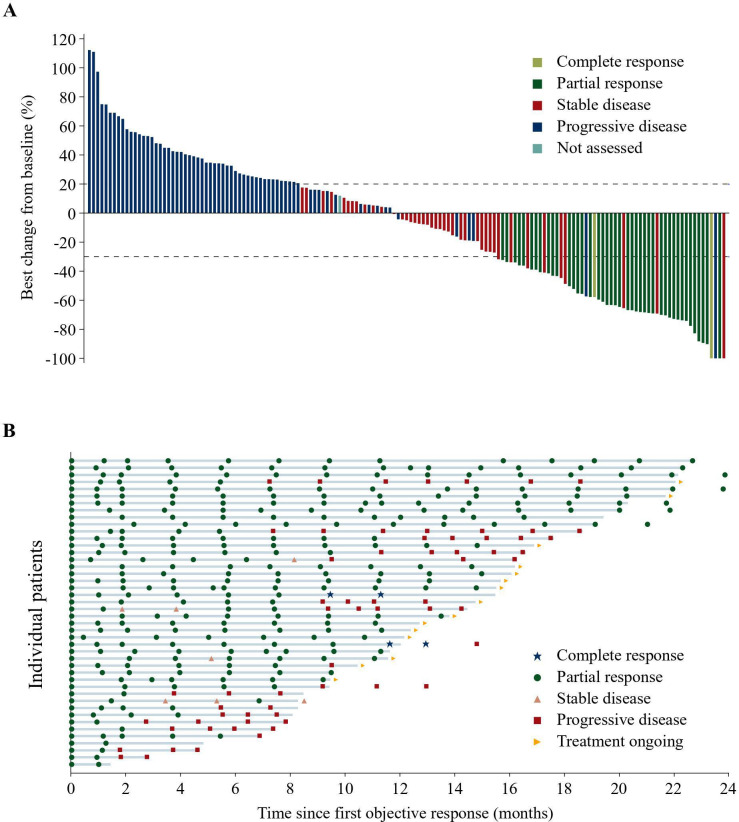
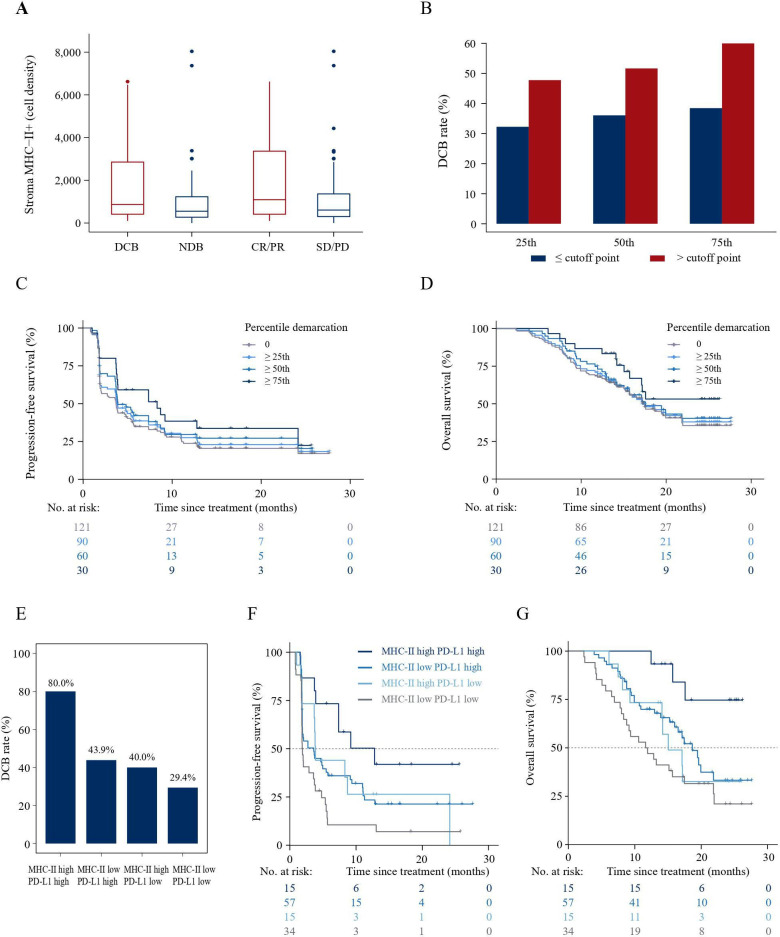
Between August 14, 2018, and December 30, 2019, a total of 156 patients were enrolled. The IRC-assessed ORR was 28.2% (95% CI 21.3% to 36.0%). The median progression-free survival was 3.7 months (95% CI 2.0 to 4.1) per IRC, and the median overall survival was 17.4 months (95% CI 15.2 to 21.9). The ORRs were 35.2% (95% CI 25.3% to 46.1%) vs 19.4% (95% CI 10.4% to 31.4%) in patients with tumor PD-L1 expression of ≥10% and<10%, respectively. Patients with durable clinical benefit (DCB), which was defined as complete response, partial response or stable disease of ≥18 weeks, had higher density of MHC-II+ cell in stroma than patients without DCB (median 868.1 (IQR 413.4-2854.0) cells/mm vs median 552.4 (IQR 258.4 to 1242.1) cells/mm). MHC-II+ cell density did not correlate with PD-L1 expression, and a composite of high stromal MHC-II+ cell density and tumor PD-L1 expression further enriched patients who could benefit from camrelizumab.
Camrelizumab had clinically meaningful antitumor activity in patients with recurrent or metastatic NPC. The composition of both MHC-II+ cell density and PD-L1 expression could result in better patient selection.
本研究旨在评估抗程序性死亡-1 抗体卡瑞利珠单抗在预处理后复发或转移性鼻咽癌(NPC)患者中的抗肿瘤活性,并探索预测生物标志物。
复发(不能进行局部治愈性治疗)或转移性 NPC 患者,在接受至少两线化疗后失败,有资格接受卡瑞利珠单抗(200mg,每 2 周静脉注射一次)治疗 2 年或直至疾病进展、无法耐受的不良事件、撤回同意书或研究者决定。主要终点为独立评审委员会(IRC)评估的客观缓解率(ORR)。通过免疫组织化学法评估程序性死亡配体 1(PD-L1)表达。通过多重免疫荧光染色评估其他免疫相关生物标志物,包括主要组织相容性复合体 I 和 II(MHC-II)。
2018 年 8 月 14 日至 2019 年 12 月 30 日期间,共纳入 156 例患者。IRC 评估的 ORR 为 28.2%(95%CI,21.3%至 36.0%)。IRC 评估的中位无进展生存期为 3.7 个月(95%CI,2.0 至 4.1),中位总生存期为 17.4 个月(95%CI,15.2 至 21.9)。肿瘤 PD-L1 表达≥10%和<10%的患者的 ORR 分别为 35.2%(95%CI,25.3%至 46.1%)和 19.4%(95%CI,10.4%至 31.4%)。具有持久临床获益(DCB)的患者,定义为完全缓解、部分缓解或稳定疾病≥18 周,其基质中 MHC-II+细胞密度高于无 DCB 的患者(中位数 868.1(IQR,413.4-2854.0)个/mm 与中位数 552.4(IQR,258.4 至 1242.1)个/mm)。MHC-II+细胞密度与 PD-L1 表达不相关,而高基质 MHC-II+细胞密度和肿瘤 PD-L1 表达的组合可进一步富集可从卡瑞利珠单抗中获益的患者。
卡瑞利珠单抗在复发或转移性 NPC 患者中具有临床意义的抗肿瘤活性。MHC-II+细胞密度和 PD-L1 表达的组合可能导致更好的患者选择。