Department of Neurology and Stroke Center University Hospital Basel and University of Basel Basel Switzerland.
Clinical Trial Unit University of Basel Switzerland.
J Am Heart Assoc. 2022 Jan 4;11(1):e023345. doi: 10.1161/JAHA.121.023345. Epub 2021 Dec 22.
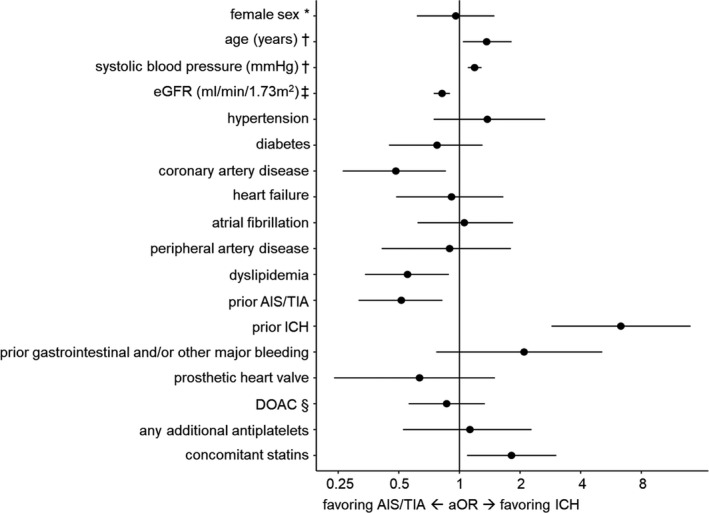
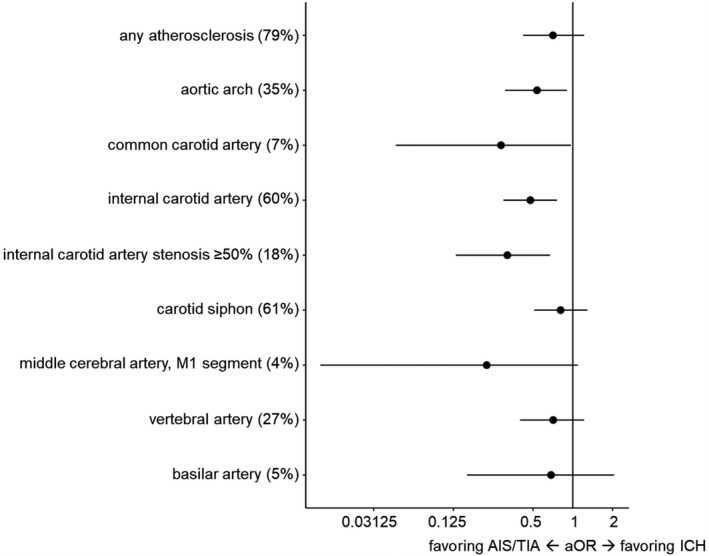
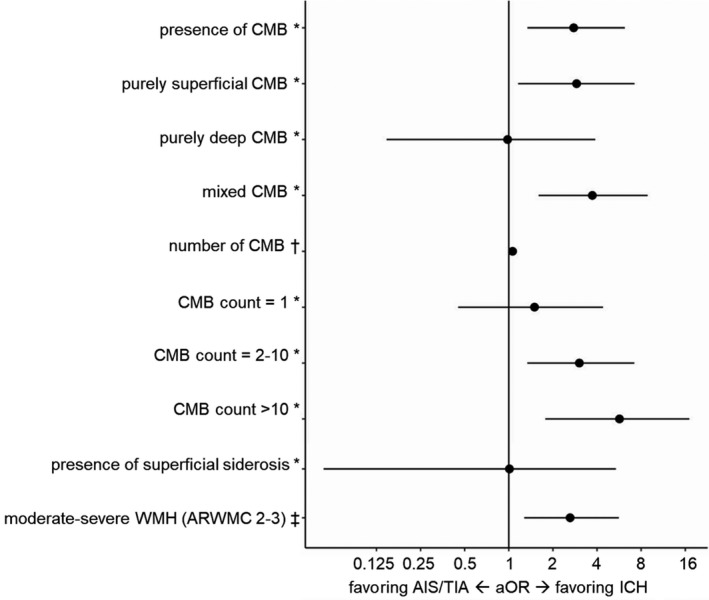
Background Data on the relative contribution of clinical and neuroimaging risk factors to acute ischemic stroke (AIS) versus intracerebral hemorrhage (ICH) occurring on oral anticoagulant treatment are scarce. Methods and Results Cross-sectional study was done on consecutive oral anticoagulant-treated patients presenting with AIS, transient ischemic attack (TIA), or ICH from the prospective observational NOACISP (Novel-Oral-Anticoagulants-In-Stroke-Patients)-Acute registry. We compared clinical and neuroimaging characteristics (small vessel disease markers and atherosclerosis) in ICH versus AIS/TIA (reference) using logistic regression. Among 734 patients presenting with stroke on oral anticoagulant treatment (404 [55%] direct oral anticoagulants, 330 [45%] vitamin K antagonists), 605 patients (82%) had AIS/TIA and 129 (18%) had ICH. Prior AIS/TIA, coronary artery disease, dyslipidemia, and worse renal function were associated with AIS/TIA (adjusted odds ratio [aOR] [95% CI] 0.51 [0.32-0.82], 0.48 [0.26-0.86], 0.55 [0.34-0.89], and 0.82 [0.75-0.90] per 10 mL/min). Prior ICH, older age, higher admission blood pressure, and statin treatment were associated with ICH (aOR [95% CI] 6.33 [2.87-14.04], 1.37 [1.04-1.81] per 10 years, 1.19 [1.10-1.29] per 10 mm Hg, and 1.81 [1.09-3.03]). Cerebral microbleeds and moderate-to-severe white matter hyperintensities contributed more to ICH (aOR [95% CI] 2.77 [1.34-6.18], and 2.62 [1.28-5.63]). Aortic arch, common and internal carotid artery atherosclerosis, and internal carotid artery stenosis ≥50% contributed more to AIS/TIA (aOR [95% CI] 0.54 [0.31-0.90], 0.29 [0.05-0.97], 0.48 [0.30-0.76], and 0.32 [0.13-0.67]). Conclusions In patients presenting with stroke on oral anticoagulant, AIS/TIA was 5 times more common than ICH. A high atherosclerotic burden (indicated by cardiovascular comorbidities and extracranial atherosclerosis) and prior AIS/TIA contributed more to AIS/TIA, while small vessel disease markers and prior ICH were stronger determinants for ICH. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02353585.
背景 关于在接受口服抗凝剂治疗时发生的急性缺血性卒中(AIS)与颅内出血(ICH)中临床和神经影像学危险因素相对贡献的数据很少。
方法 我们对来自前瞻性观察性 NOACISP(新型口服抗凝剂在卒中患者中的研究)急性登记处的连续接受口服抗凝剂治疗并出现 AIS、短暂性脑缺血发作(TIA)或 ICH 的口服抗凝剂治疗患者进行了横断面研究。我们使用逻辑回归比较了 ICH 与 AIS/TIA(参考)的临床和神经影像学特征(小血管疾病标志物和动脉粥样硬化)。在 734 名接受口服抗凝剂治疗的卒中患者中(404 名[55%]直接口服抗凝剂,330 名[45%]维生素 K 拮抗剂),605 名(82%)为 AIS/TIA,129 名(18%)为 ICH。既往 AIS/TIA、冠心病、血脂异常和肾功能恶化与 AIS/TIA 相关(调整后的比值比 [aOR] [95%CI] 0.51 [0.32-0.82]、0.48 [0.26-0.86]、0.55 [0.34-0.89] 和 0.82 [0.75-0.90]每 10ml/min)。既往 ICH、年龄较大、入院血压较高和他汀类药物治疗与 ICH 相关(aOR [95%CI] 6.33 [2.87-14.04]、每 10 岁 1.37 [1.04-1.81]、每 10mmHg 1.19 [1.10-1.29] 和 1.81 [1.09-3.03])。脑微出血和中重度脑白质高信号与 ICH 关系更密切(aOR [95%CI] 2.77 [1.34-6.18]和 2.62 [1.28-5.63])。主动脉弓、颈总动脉和颈内动脉粥样硬化以及颈内动脉狭窄≥50%与 AIS/TIA 关系更密切(aOR [95%CI] 0.54 [0.31-0.90]、0.29 [0.05-0.97]、0.48 [0.30-0.76] 和 0.32 [0.13-0.67])。
结论 在接受口服抗凝剂治疗的卒中患者中,AIS/TIA 比 ICH 常见 5 倍。高动脉粥样硬化负荷(由心血管合并症和颅外动脉粥样硬化指示)和既往 AIS/TIA 与 AIS/TIA 关系更密切,而小血管疾病标志物和既往 ICH 是 ICH 的更强决定因素。