Department of Ultrasound, The Second Affiliated Hospital of Soochow University, 1055 Sanxiang Road, Suzhou, Jiangsu, China.
Department of Urology, The Second Affiliated Hospital of Soochow University, 1055 Sanxiang Road, Suzhou, Jiangsu, China.
BMC Urol. 2021 Dec 23;21(1):183. doi: 10.1186/s12894-021-00949-7.
Combining targeted biopsy (TB) with systematic biopsy (SB) is currently recommended as the first-line biopsy method by the European Association of Urology (EAU) guidelines in patients diagnosed with prostate cancer (PCa) with an abnormal magnetic resonance imaging (MRI). The combined SB and TB indeed detected an additional number of patients with clinically significant prostate cancer (csPCa); however, it did so at the expense of a concomitant increase in biopsy cores. Our study aimed to evaluate if ipsilateral SB (ipsi-SB) + TB or contralateral SB (contra-SB) + TB could achieve almost equal csPCa detection rates as SB + TB using fewer cores based on a different csPCa definition.
Patients with at least one positive prostate lesion were prospectively diagnosed by MRI. The combination of TB and SB was conducted in all patients. We compared the csPCa detection rates of the following four hypothetical biopsy sampling schemes with those of SB + TB: SB, TB, ipsi-SB + TB, and contra-SB + TB.
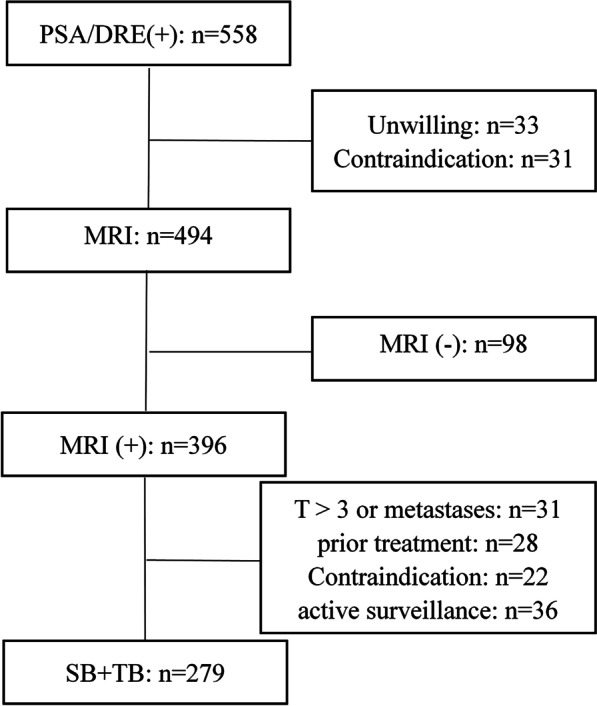
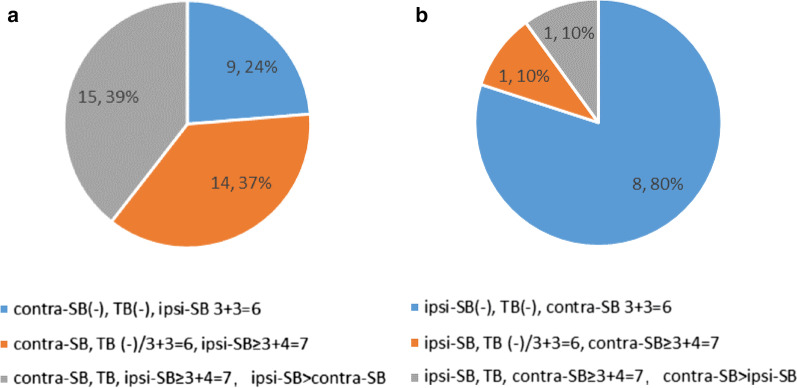
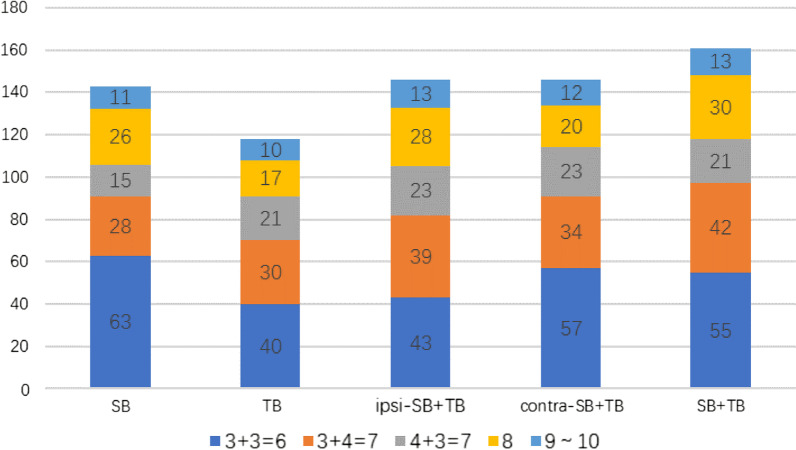
The study enrolled 279 men. The median core of SB, TB, ipsi-SB + TB, and contra-SB + TB was 10, 2, 7 and 7, respectively (P < 0.001). ipsi-SB + TB detected significantly more patients with csPCa than contra-SB + TB based on the EAU guidelines (P = 0.042). They were almost equal on the basis of the Epstein criteria (P = 1.000). Compared with SB + TB, each remaining method detected significantly fewer patients with csPCa regardless of the definition (P < 0.001) except ipsi-SB + TB on the grounds of D1 (P = 0.066). Ten additional subjects were identified with a higher Gleason score (GS) on contra-SB + TB, and only one was considered as significantly upgraded (GS = 6 on ipsi-SB + TB to a GS of 8 on contra-SB + TB).
Ipsi-SB + TB could acquire an almost equivalent csPCa detection value to SB + TB using significantly fewer cores when csPCa was defined according to the EAU guidelines. Given that there was only one significantly upgrading patient on contra-SB, our results suggested that contra-SB could be avoided.
目前,欧洲泌尿外科学会(EAU)指南建议,对于磁共振成像(MRI)异常的前列腺癌(PCa)患者,将靶向活检(TB)与系统活检(SB)相结合作为一线活检方法。联合 SB 和 TB 确实可以检测到更多患有临床显著前列腺癌(csPCa)的患者;然而,这是以增加活检核心数为代价的。我们的研究旨在评估同侧 SB(ipsi-SB)+TB 或对侧 SB(contra-SB)+TB 是否可以使用更少的核心数,基于不同的 csPCa 定义,达到与 SB+TB 几乎相同的 csPCa 检出率。
前瞻性诊断至少有一个阳性前列腺病变的患者。所有患者均行 TB 和 SB 联合检查。我们比较了以下四种假设的活检采样方案与 SB+TB 的 csPCa 检出率:SB、TB、ipsi-SB+TB 和 contra-SB+TB。
该研究共纳入 279 名男性。SB、TB、ipsi-SB+TB 和 contra-SB+TB 的中位活检核心数分别为 10、2、7 和 7(P<0.001)。根据 EAU 指南,ipsi-SB+TB 比 contra-SB+TB 检测到更多的 csPCa 患者(P=0.042)。根据 Epstein 标准,它们几乎相等(P=1.000)。与 SB+TB 相比,无论采用何种定义,其余每种方法检测到的 csPCa 患者均显著减少(P<0.001),但基于 D1 的 ipsi-SB+TB 除外(P=0.066)。在 contra-SB+TB 上发现了 10 例 Gleason 评分(GS)更高的附加病例,只有 1 例被认为是明显升级(ipsi-SB+TB 的 GS=6 升级到 contra-SB+TB 的 GS=8)。
当根据 EAU 指南定义 csPCa 时,ipsi-SB+TB 可以使用显著更少的核心数获得与 SB+TB 几乎相等的 csPCa 检出值。鉴于 contra-SB 上只有 1 例明显升级的患者,我们的结果表明可以避免对侧 SB。