See Hoe Louise E, Wildi Karin, Obonyo Nchafatso G, Bartnikowski Nicole, McDonald Charles, Sato Kei, Heinsar Silver, Engkilde-Pedersen Sanne, Diab Sara, Passmore Margaret R, Wells Matthew A, Boon Ai-Ching, Esguerra Arlanna, Platts David G, James Lynnette, Bouquet Mahe, Hyslop Kieran, Shuker Tristan, Ainola Carmen, Colombo Sebastiano M, Wilson Emily S, Millar Jonathan E, Malfertheiner Maximillian V, Reid Janice D, O'Neill Hollier, Livingstone Samantha, Abbate Gabriella, Sato Noriko, He Ting, von Bahr Viktor, Rozencwajg Sacha, Byrne Liam, Pimenta Leticia P, Marshall Lachlan, Nair Lawrie, Tung John-Paul, Chan Jonathan, Haqqani Haris, Molenaar Peter, Li Bassi Gianluigi, Suen Jacky Y, McGiffin David C, Fraser John F
Critical Care Research Group, The Prince Charles Hospital, Brisbane, QLD, Australia.
Prince Charles Hospital Northside Clinical Unit, Faculty of Medicine, University of Queensland, Brisbane, QLD, Australia.
Intensive Care Med Exp. 2021 Dec 24;9(1):60. doi: 10.1186/s40635-021-00425-4.
Heart transplantation (HTx) from brainstem dead (BSD) donors is the gold-standard therapy for severe/end-stage cardiac disease, but is limited by a global donor heart shortage. Consequently, innovative solutions to increase donor heart availability and utilisation are rapidly expanding. Clinically relevant preclinical models are essential for evaluating interventions for human translation, yet few exist that accurately mimic all key HTx components, incorporating injuries beginning in the donor, through to the recipient. To enable future assessment of novel perfusion technologies in our research program, we thus aimed to develop a clinically relevant sheep model of HTx following 24 h of donor BSD.
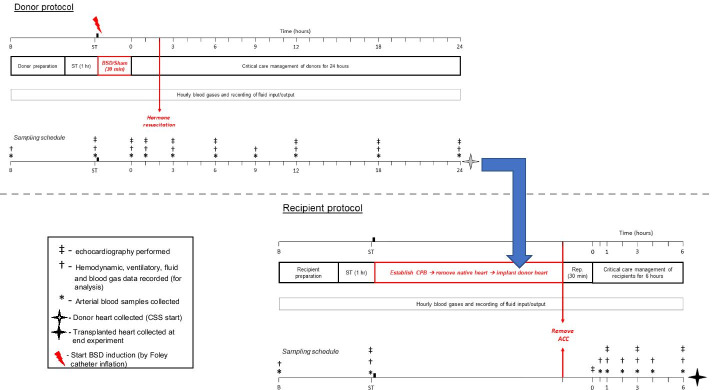
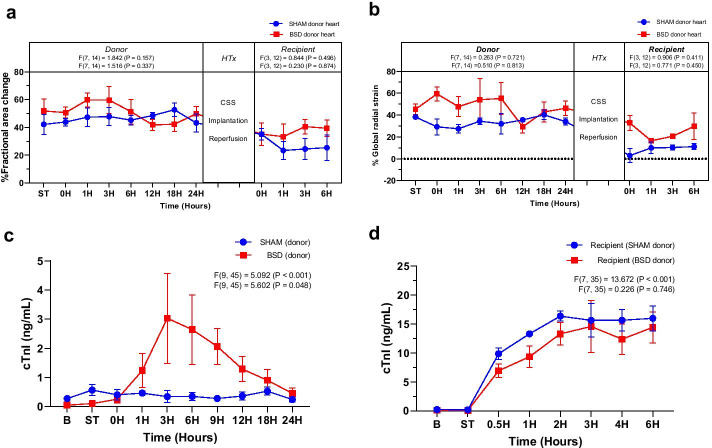
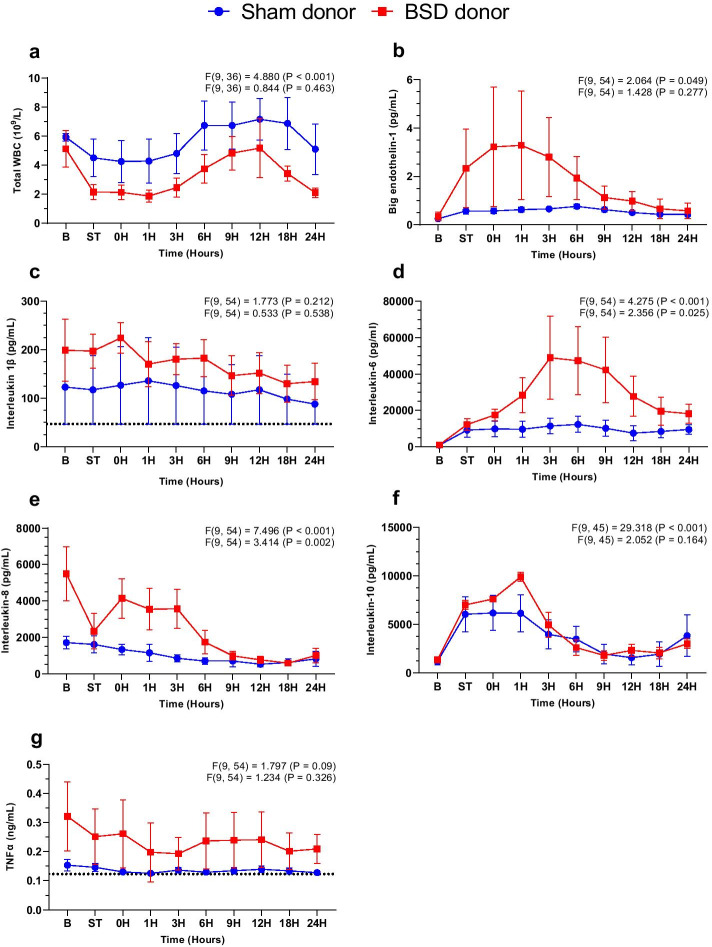
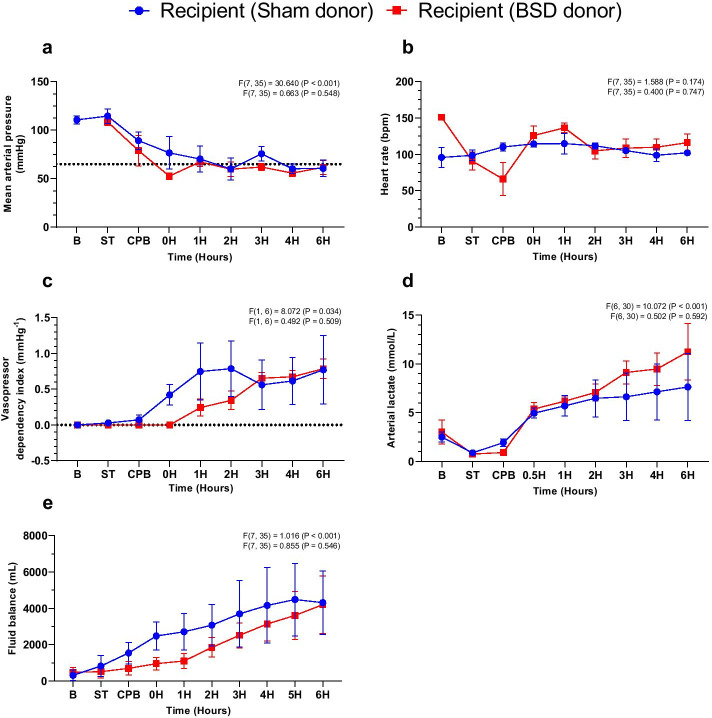
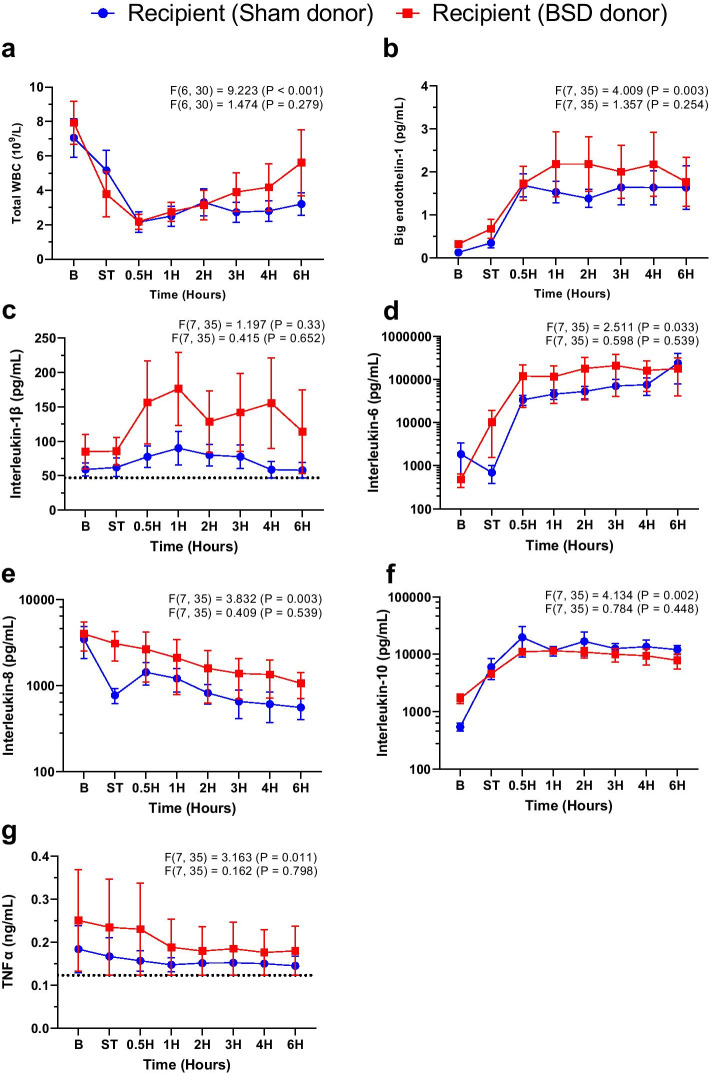
BSD donors (vs. sham neurological injury, 4/group) were hemodynamically supported and monitored for 24 h, followed by heart preservation with cold static storage. Bicaval orthotopic HTx was performed in matched recipients, who were weaned from cardiopulmonary bypass (CPB), and monitored for 6 h. Donor and recipient blood were assayed for inflammatory and cardiac injury markers, and cardiac function was assessed using echocardiography. Repeated measurements between the two different groups during the study observation period were assessed by mixed ANOVA for repeated measures.
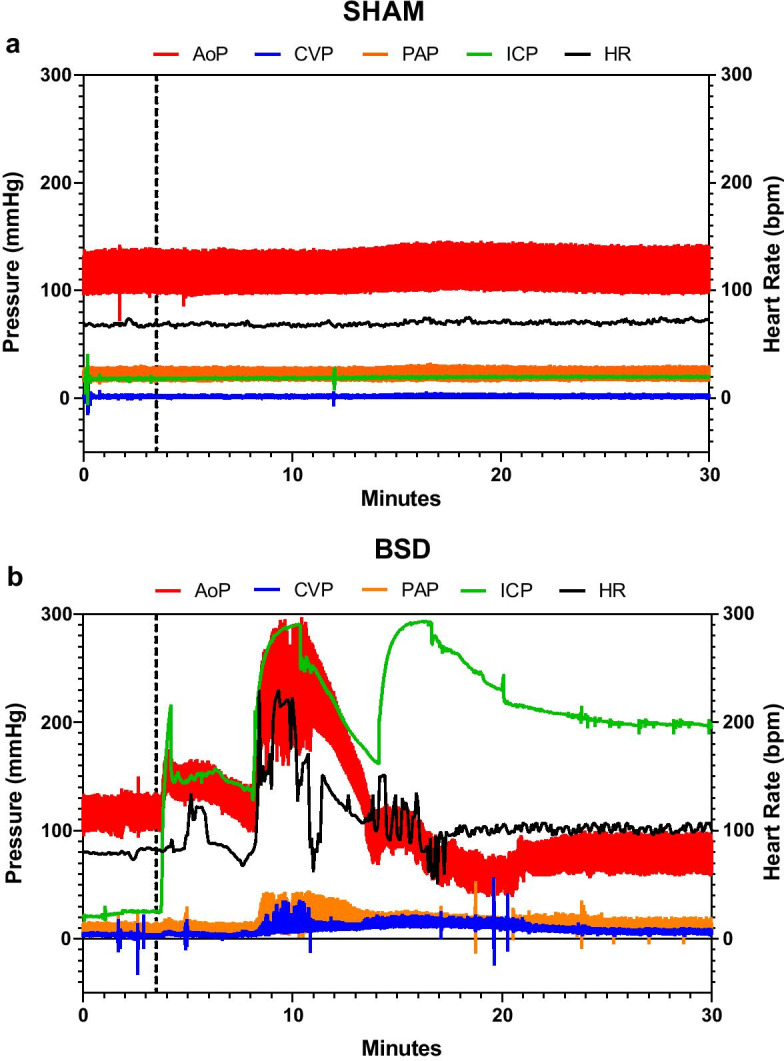
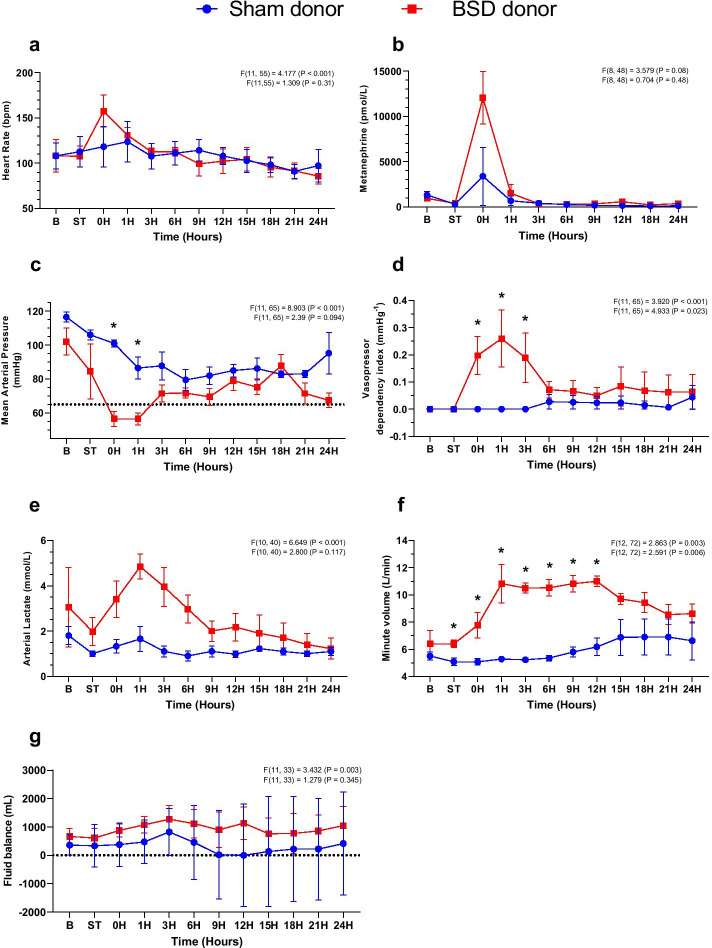
Brainstem death caused an immediate catecholaminergic hemodynamic response (mean arterial pressure, p = 0.09), systemic inflammation (IL-6 - p = 0.025, IL-8 - p = 0.002) and cardiac injury (cardiac troponin I, p = 0.048), requiring vasopressor support (vasopressor dependency index, VDI, p = 0.023), with normalisation of biomarkers and physiology over 24 h. All hearts were weaned from CPB and monitored for 6 h post-HTx, except one (sham) recipient that died 2 h post-HTx. Hemodynamic (VDI - p = 0.592, heart rate - p = 0.747) and metabolic (blood lactate, p = 0.546) parameters post-HTx were comparable between groups, despite the observed physiological perturbations that occurred during donor BSD. All p values denote interaction among groups and time in the ANOVA for repeated measures.
We have successfully developed an ovine HTx model following 24 h of donor BSD. After 6 h of critical care management post-HTx, there were no differences between groups, despite evident hemodynamic perturbations, systemic inflammation, and cardiac injury observed during donor BSD. This preclinical model provides a platform for critical assessment of injury development pre- and post-HTx, and novel therapeutic evaluation.
来自脑死亡(BSD)供体的心脏移植(HTx)是治疗严重/终末期心脏病的金标准疗法,但受到全球供体心脏短缺的限制。因此,增加供体心脏可用性和利用率的创新解决方案正在迅速扩展。临床相关的临床前模型对于评估用于人体转化的干预措施至关重要,但很少有模型能准确模拟HTx的所有关键组成部分,包括从供体开始到受体的损伤。为了在我们的研究项目中能够对新型灌注技术进行未来评估,我们旨在建立一个在供体BSD 24小时后进行HTx的临床相关绵羊模型。
对BSD供体(与假神经损伤组相比,每组4只)进行血流动力学支持并监测24小时,然后用冷静态保存法保存心脏。在匹配的受体中进行双腔原位HTx,受体脱离体外循环(CPB),并监测6小时。检测供体和受体血液中的炎症和心脏损伤标志物,并使用超声心动图评估心脏功能。在研究观察期内,对两组之间的重复测量采用重复测量的混合方差分析进行评估。
脑死亡引起了立即的儿茶酚胺能血流动力学反应(平均动脉压,p = 0.09)、全身炎症(IL-6 - p = 0.025,IL-8 - p = 0.002)和心脏损伤(心肌肌钙蛋白I,p = 0.048),需要血管升压药支持(血管升压药依赖指数,VDI,p = 0.023),生物标志物和生理指标在24小时内恢复正常。除1只(假手术)受体在HTx后2小时死亡外,所有心脏均脱离CPB并在HTx后监测6小时。尽管在供体BSD期间观察到生理扰动,但HTx后两组的血流动力学(VDI - p = 0.592,心率 - p = 0.747)和代谢(血乳酸,p = 0.546)参数相当。所有p值表示重复测量方差分析中组间和时间的相互作用。
我们成功建立了一个在供体BSD 24小时后进行绵羊HTx的模型。HTx后经过6小时的重症监护管理,尽管在供体BSD期间观察到明显的血流动力学扰动、全身炎症和心脏损伤,但两组之间没有差异。这个临床前模型为HTx前后损伤发展的关键评估和新型治疗评估提供了一个平台。