Department of Medical Oncology, Lung Cancer and Gastrointestinal Unit, Hunan Cancer Hospital/The Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, China; Graduate School, University of South China, Hengyang, Hunan, China.
Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
ESMO Open. 2022 Feb;7(1):100347. doi: 10.1016/j.esmoop.2021.100347. Epub 2021 Dec 23.
Approximately 2%-8% of non-small-cell lung cancer (NSCLC) harbors concurrent epidermal growth factor receptor (EGFR) sensitizing mutation and mesenchymal-epithelial transition factor (MET) amplification prior to EGFR-tyrosine kinase inhibitor (EGFR-TKI) therapy. This study aimed to investigate the optimal first-line therapeutic options for patients with concurrent EGFR-mutant, MET-overexpressed/amplified advanced NSCLC.
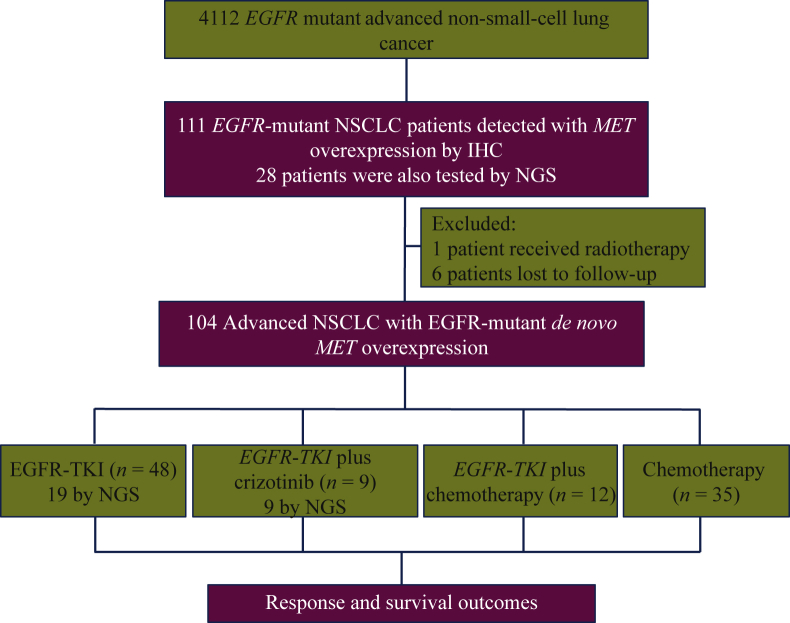
A total of 104 treatment-naïve patients with EGFR-mutant de novo MET-overexpressed advanced NSCLC were identified using immunohistochemistry and stratified to four groups according to treatment regimen: EGFR-TKI monotherapy (n = 48), EGFR-TKI combined with either crizotinib (n = 9) or chemotherapy (n = 12), and chemotherapy (n = 35). A subpopulation of 28 patients was also tested with next-generation sequencing (NGS). Objective response rate (ORR) and progression-free survival (PFS) outcomes were analyzed according to treatment strategies and molecular features.
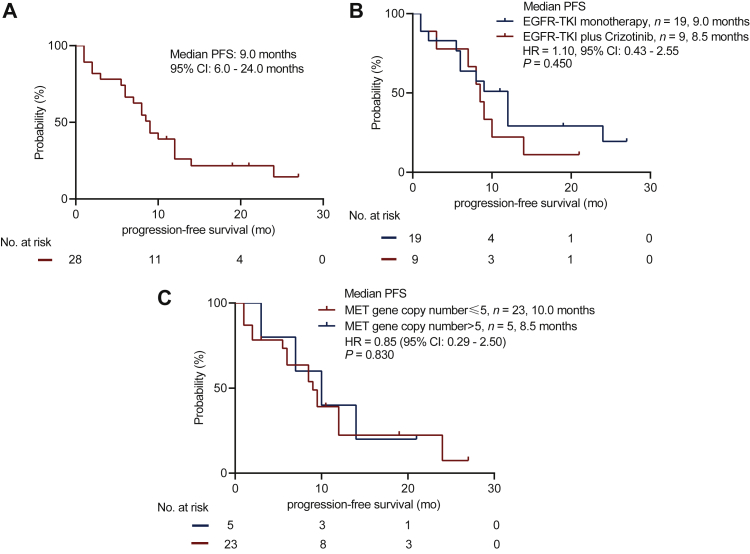
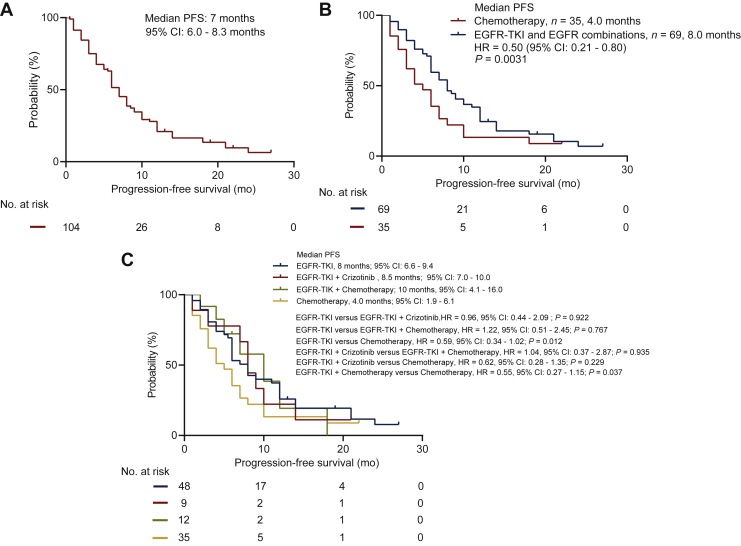
All the patients (n = 104) achieved ORR of 36.5% and median PFS (mPFS) of 7.0 months. Baseline clinicopathologic characteristics were similar among the four treatment groups. Compared with chemotherapy, EGFR-TKI monotherapy or EGFR-TKI combination therapy achieved significantly higher ORR (P < 0.001) and longer mPFS (P = 0.003). No ORR or PFS difference was observed between EGFR-TKI monotherapy and combination therapy. In the NGS-identified population (n = 28), patients who received EGFR-TKI plus crizotinib (n = 9) achieved similar ORR (88.9% versus 57.9%, P = 0.195) and mPFS (9.0 versus 8.5 months, hazard ratio 1.10, 95% confidence interval 0.43-2.55, P = 0.45) than those who received EGFR-TKI monotherapy (n = 19), regardless of MET copy number status. Grade 3/4 rashes were significantly more among patients who received EGFR-TKI plus crizotinib (P = 0.026).
Our findings provided clinical evidence that patients with concurrent EGFR sensitizing mutation and de novo MET amplification/overexpression could benefit from first-line EGFR-TKI monotherapy.
在接受表皮生长因子受体(EGFR)酪氨酸激酶抑制剂(EGFR-TKI)治疗之前,约有 2%-8%的非小细胞肺癌(NSCLC)存在并发的 EGFR 敏感突变和间充质上皮转化因子(MET)扩增。本研究旨在探讨同时存在 EGFR 突变和 MET 过表达/扩增的晚期 NSCLC 患者的最佳一线治疗选择。
使用免疫组织化学法共鉴定了 104 例 EGFR 突变的初治新发 MET 过表达晚期 NSCLC 患者,并根据治疗方案分为四组:EGFR-TKI 单药治疗(n=48)、EGFR-TKI 联合克唑替尼(n=9)或化疗(n=12)治疗、化疗(n=35)。还对 28 例患者进行了下一代测序(NGS)检测。根据治疗策略和分子特征分析客观缓解率(ORR)和无进展生存期(PFS)。
所有患者(n=104)的 ORR 为 36.5%,中位 PFS(mPFS)为 7.0 个月。四组治疗的基线临床病理特征相似。与化疗相比,EGFR-TKI 单药或联合治疗的 ORR(P<0.001)和 mPFS(P=0.003)显著更高。EGFR-TKI 单药和联合治疗之间未观察到 ORR 或 PFS 差异。在 NGS 鉴定的人群(n=28)中,接受 EGFR-TKI 加克唑替尼(n=9)治疗的患者与接受 EGFR-TKI 单药治疗(n=19)的患者 ORR(88.9%对 57.9%,P=0.195)和 mPFS(9.0 对 8.5 个月,危险比 1.10,95%置信区间 0.43-2.55,P=0.45)相似,而不论 MET 拷贝数状态如何。接受 EGFR-TKI 加克唑替尼治疗的患者中,3/4 级皮疹明显更多(P=0.026)。
我们的研究结果提供了临床证据,表明同时存在 EGFR 致敏突变和新发 MET 扩增/过表达的患者可从一线 EGFR-TKI 单药治疗中获益。