Formerly AstraZeneca, Wilmington, DE, USA.
Analysis Group, Inc., 111 Huntington Avenue, 14th Floor, Boston, MA, 02199, USA.
Adv Ther. 2022 Feb;39(2):1033-1044. doi: 10.1007/s12325-021-02017-w. Epub 2021 Dec 27.
Hyperkalemia is often managed in the emergency department (ED) and it is important to understand how ED management and post-discharge outcomes vary by hyperkalemia severity. This study was conducted to characterize ED management and post-discharge outcomes across hyperkalemia severities.
Adults with an ED visit with hyperkalemia (at least one serum potassium lab measure above 5.0 mEq/L) were selected from US electronic medical record data (2012-2018). Patient characteristics, potassium levels, treatments, and monitoring prior to and during the ED visit were compared by hyperkalemia severity (mild [> 5.0-5.5 mEq/L], moderate [> 5.5-6.0], severe [> 6.0]) using unadjusted analyses. Death, immediate inpatient admission, 30-day hyperkalemia recurrence, and 30-day inpatient admission were also assessed by severity.
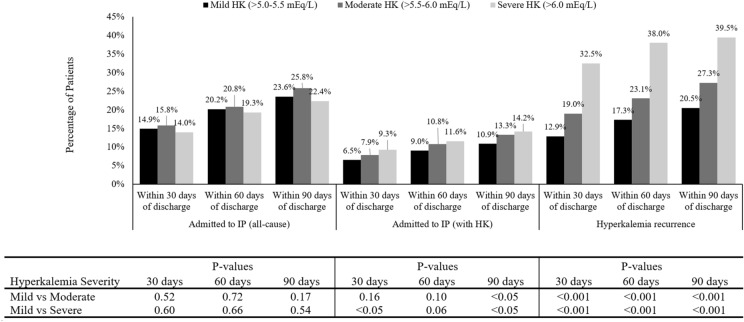
Of 6222 patients included, 4432 (71.2%) had mild hyperkalemia, 1085 (17.4%) had moderate, and 705 (11.3%) had severe hyperkalemia. Chronic kidney disease (39.9-50.1%) and heart failure (21.6-24.3%) were common. In the ED, electrocardiograms (mild, 56.5%; moderate, 69.6%; severe, 81.0%) and patients with at least two potassium laboratory values increased with severity (15.0%; 40.4%; 75.5%). Among patients with at least two potassium laboratory values, over half of patients (60.4%) had potassium levels ≤ 5.0 mEq/L prior to discharge. Use of potassium-binding treatments (sodium polystyrene sulfonate: mild = 4.1%; moderate = 17.1%; severe = 27.4%), temporizing agents (5.6%; 15.5%; 31.6%), or dialysis (0.4%; 0.8%; 3.0%) increased with severity; treatment at discharge was not common. Death (1.1%; 3.7%; 10.6%), immediate admission to inpatient care (5.8%; 8.7%; 12.7%), 30-day hyperkalemia recurrence (2.9%; 19.0%; 32.5%), 30-day inpatient admission with hyperkalemia (6.5%; 7.9%; 9.3%) also increased with severity.
Patients with moderate and severe hyperkalemia experienced elevated risk of hyperkalemia recurrence and hyperkalemia-related inpatient readmission following discharge from the ED from a descriptive analysis. Future research to assess strategies to reduce hyperkalemia recurrence and inpatient admission in this patient population would be beneficial.
高钾血症通常在急诊科(ED)进行治疗,了解 ED 管理和出院后结局如何因高钾血症的严重程度而变化非常重要。本研究旨在描述不同严重程度高钾血症患者的 ED 管理和出院后结局。
从美国电子病历数据(2012-2018 年)中选择 ED 就诊伴有高钾血症(至少有一次血清钾检测值高于 5.0 mEq/L)的成年患者。使用未调整的分析方法,根据高钾血症的严重程度(轻度[>5.0-5.5 mEq/L]、中度[>5.5-6.0]、重度[>6.0])比较患者特征、钾水平、治疗方法以及 ED 就诊前后的监测情况。还根据严重程度评估了死亡、即刻住院、30 天内高钾血症复发和 30 天内住院情况。
在纳入的 6222 例患者中,4432 例(71.2%)为轻度高钾血症,1085 例(17.4%)为中度高钾血症,705 例(11.3%)为重度高钾血症。慢性肾脏病(39.9-50.1%)和心力衰竭(21.6-24.3%)很常见。在 ED 中,心电图(轻度 56.5%;中度 69.6%;重度 81.0%)和至少两次血钾实验室值升高与严重程度相关(15.0%;40.4%;75.5%)。在至少两次血钾实验室值的患者中,超过一半的患者(60.4%)在出院前血钾水平≤5.0 mEq/L。使用钾结合治疗药物(聚苯乙烯磺酸钠:轻度 4.1%;中度 17.1%;重度 27.4%)、临时治疗药物(5.6%;15.5%;31.6%)或透析(0.4%;0.8%;3.0%)的患者比例随严重程度增加而增加;出院时的治疗并不常见。死亡(1.1%;3.7%;10.6%)、立即入院治疗(5.8%;8.7%;12.7%)、30 天内高钾血症复发(2.9%;19.0%;32.5%)、30 天内因高钾血症再次住院(6.5%;7.9%;9.3%)也随严重程度增加而增加。
描述性分析显示,中度和重度高钾血症患者在 ED 出院后发生高钾血症复发和高钾血症相关住院的风险增加。未来评估减少该患者人群中高钾血症复发和住院的策略的研究将是有益的。