Timmermann Lea, Globke Brigitta, Lurje Georg, Schmelzle Moritz, Schöning Wenzel, Öllinger Robert, Pratschke Johann, Eberspächer Bettina, Drosten Christian, Hofmann Jörg, Eurich Dennis
Department of Surgery, Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, 13353 Berlin, Germany.
Labor Berlin-Charité Vivantes GmbH, 13353 Berlin, Germany.
Vaccines (Basel). 2021 Dec 1;9(12):1422. doi: 10.3390/vaccines9121422.
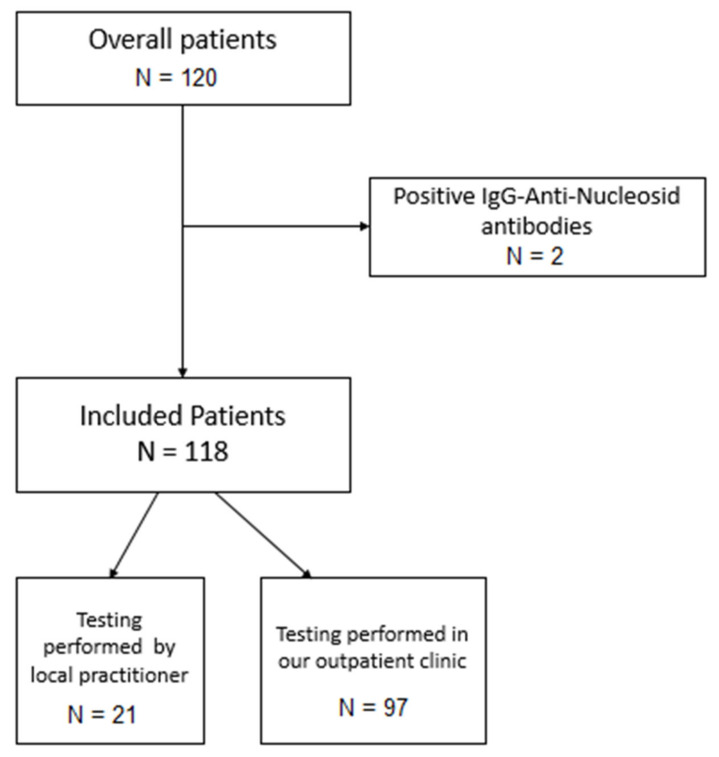
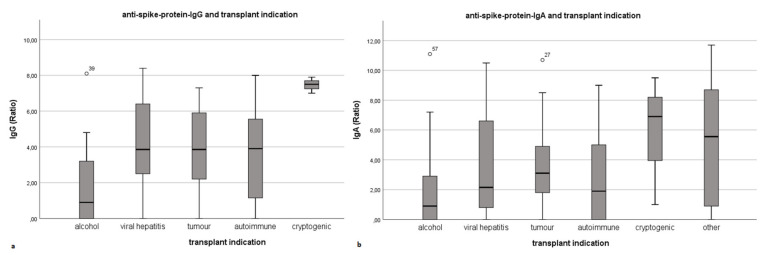
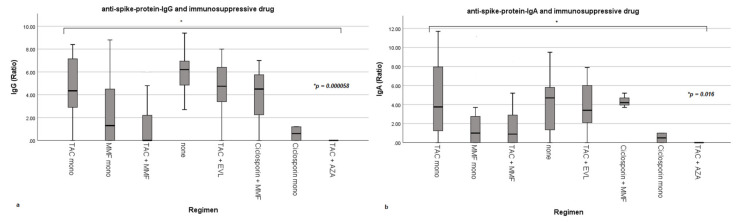
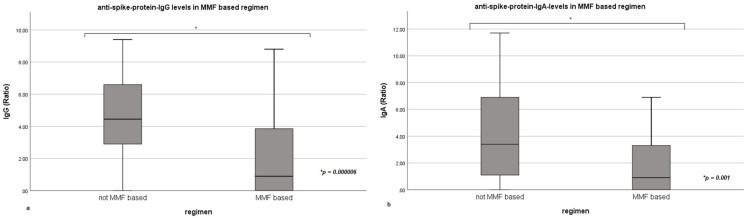
As COVID-19 remains an issue in transplantation medicine, a successful vaccination can prevent infections and life-threatening courses. The probability of poor immune response in liver transplant recipients gained attention and insecurity among those patients, leading us to investigate the humoral immune response alongside the influence of underlying diseases and immunosuppressive regimen on seroconversion rates. We included 118 patients undergoing anti-spike-protein-IgG testing at least 21 days after completed SARS-CoV-2 vaccination. Ninety-seven patients also underwent anti-spike-protein-IgA testing. The influence of baseline demographics, immunosuppressive regimen and underlying disease on seroconversion was analyzed, and 92 of 118 patients (78.0%) developed anti-spike-protein-IgG antibodies. Patients with a history of alcoholic liver disease before transplantation showed significantly lower seroconversion rates ( = 0.006). Immunosuppression also significantly influenced antibody development ( < 0.001). Patients run on a mycophenolate mofetil (MMF)-based regimen were more likely not to develop antibodies compared to patients run on a non-MMF regimen ( < 0.001). All patients weaned off immunosuppression were seropositive. The seroconversion rate of 78.0% in our cohort of liver transplant recipients is promising. The identification of alcohol-induced cirrhosis as underlying disease and MMF for immunosuppression as risk factors for seronegativity may serve to identify vaccination non-responder after liver transplantation.
由于新冠病毒病(COVID-19)仍是移植医学中的一个问题,成功接种疫苗可预防感染和危及生命的病程。肝移植受者免疫反应不佳的可能性引起了这些患者的关注和不安,促使我们研究体液免疫反应以及基础疾病和免疫抑制方案对血清转化阳性率的影响。我们纳入了118例在完成新冠病毒2(SARS-CoV-2)疫苗接种至少21天后接受抗刺突蛋白IgG检测的患者。97例患者还接受了抗刺突蛋白IgA检测。分析了基线人口统计学、免疫抑制方案和基础疾病对血清转化的影响,118例患者中有92例(78.0%)产生了抗刺突蛋白IgG抗体。移植前有酒精性肝病病史的患者血清转化阳性率显著较低(P = 0.006)。免疫抑制也显著影响抗体产生(P < 0.001)。与接受非霉酚酸酯(MMF)方案的患者相比,接受基于MMF方案的患者更有可能不产生抗体(P < 0.001)。所有停用免疫抑制的患者血清学均为阳性。我们肝移植受者队列中78.0%的血清转化阳性率很有前景。将酒精性肝硬化确定为基础疾病以及将MMF用于免疫抑制确定为血清学阴性的危险因素,可能有助于识别肝移植后的疫苗接种无反应者。