Department of Trauma and Orthopaedic Surgery, University Medical Center Hamburg-Eppendorf, Martinistrasse 52, 20246, Hamburg, Germany.
CLARAHOF Clinic of Orthopaedic Surgery, University of Basel, Basel, Switzerland.
Arch Orthop Trauma Surg. 2022 Dec;142(12):3917-3925. doi: 10.1007/s00402-021-04298-w. Epub 2021 Dec 28.
An increased tibial slope is a risk factor for rupture of the anterior cruciate ligament. In addition, a tibial bone bruise or posterior lateral impression associated with slope changes also poses chronic ligamentous instability of the knee joint associated with an anterior cruciate ligament (ACL) injury. In the majority of cases, the slope is measured in one plane X-ray in the lateral view. However, this does not sufficient represent the complex anatomy of the tibial plateau and especially for the posterolateral quadrant. Normal values from a "healthy" population are necessary to understand if stability of the knee joint is negatively affected by an increasing slope in the posterolateral area. Until now there are no data about the physiological slope in the posterolateral quadrant of the tibial plateau.
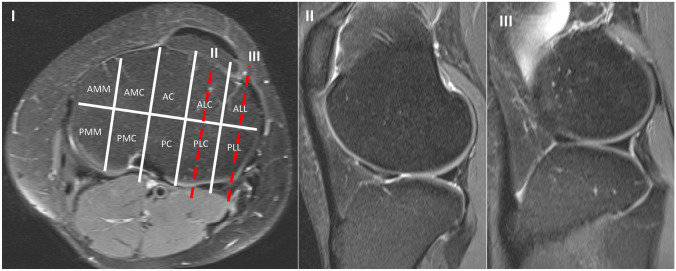
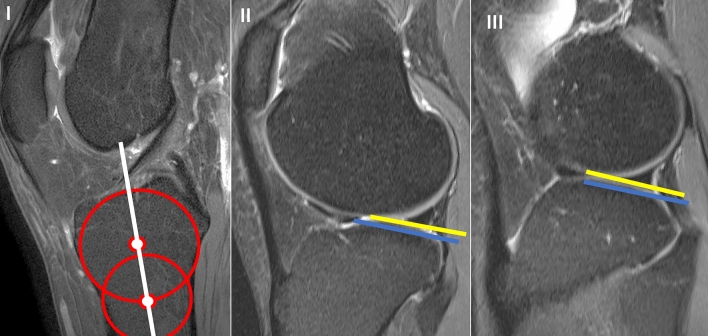
In 116 MRI scans of patients without ligamentous lesions and 116 MRI scans with an ACL rupture, tibial slope was retrospectively determined using the method described by Hudek et al. Measurements were made in the postero-latero-lateral (PLL) and postero-latero-central (PLC) segments using the 10-segment classification. In both segments, the osseous as well as the cartilaginous slope was measured. Measurements were performed by two independent surgeons.
In the group without ligamentous injury the mean bony PLL slope was 5.8° ± 4.8° and the cartilaginous PLL slope was 6.7° ± 4.8°. In the PLC segment the mean bony slope was 6.6° ± 5.0° and the cartilaginous slope was 9.4° ± 5.7°. In the cohort with ACL rupture, the bony and cartilaginous slope in both PLL and PCL were significantly higher (P < 0.001) than in the group without ACL injury (bony PLL 9.8° ± 4.8°, cartilage PLL 10.4° ± 4.7°, bony PLC 10.3° ± 4.8°, cartilage PLL 12.8° ± 4.3°). Measurements were performed independently by two experienced surgeons. There were good inter- (CI 87-98.7%) and good intraobserver (CI 85.8-99.6%) reliability.
The bony and the cartilaginous slope in the posterolateral quadrant of the tibial plateau are different but not independent. Patients with an anterior cruciate ligament injury have a significantly steeper slope in the posterolateral quadrant compared to a healthy group. Our data indicate that this anatomic feature might be a risk factor for a primary ACL injury which has not been described yet.
III.
胫骨斜率增加是前交叉韧带断裂的一个危险因素。此外,与斜率变化相关的胫骨骨挫伤或后外侧凹陷也会导致膝关节慢性韧带不稳定,与前交叉韧带(ACL)损伤有关。在大多数情况下,斜率是在外侧视图的一个平面 X 光片中测量的。然而,这并不能充分代表胫骨平台的复杂解剖结构,特别是后外侧象限。需要有“健康”人群的正常数值,才能了解后外侧区域斜率的增加是否会对膝关节的稳定性产生负面影响。到目前为止,还没有关于胫骨平台后外侧象限的生理斜率的数据。
在 116 例无韧带损伤的 MRI 扫描和 116 例 ACL 破裂的 MRI 扫描中,回顾性地使用 Hudek 等人描述的方法确定胫骨斜率。使用 10 节段分类法在后外侧-外侧(PLL)和后外侧-中央(PLC)节段测量胫骨斜率。在这两个节段中,都测量了骨性和软骨性斜率。测量由两名独立的外科医生进行。
在无韧带损伤组中,骨性 PLL 斜率的平均值为 5.8°±4.8°,软骨性 PLL 斜率的平均值为 6.7°±4.8°。在 PLC 节段,骨性斜率的平均值为 6.6°±5.0°,软骨性斜率的平均值为 9.4°±5.7°。在 ACL 破裂的队列中,PLL 和 PCL 中的骨性和软骨性斜率均明显高于无 ACL 损伤组(骨性 PLL 9.8°±4.8°,软骨 PLL 10.4°±4.7°,骨性 PLC 10.3°±4.8°,软骨 PLL 12.8°±4.3°)(P<0.001)。测量由两名经验丰富的外科医生独立进行。具有良好的组内(CI 87-98.7%)和良好的观察者内(CI 85.8-99.6%)可靠性。
胫骨平台后外侧象限的骨性和软骨性斜率不同,但不独立。与健康组相比,前交叉韧带损伤患者的后外侧象限斜率明显更陡。我们的数据表明,这种解剖特征可能是导致尚未描述的原发性 ACL 损伤的一个危险因素。
III。