New York Sport & Rehabilitation Medicine P.C, 140 Middle Neck Rd, Great Neck, NY.
Medicine (Baltimore). 2021 Nov 24;100(47):e27839. doi: 10.1097/MD.0000000000027839.
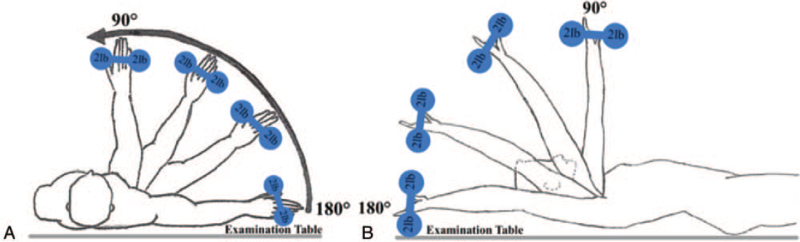
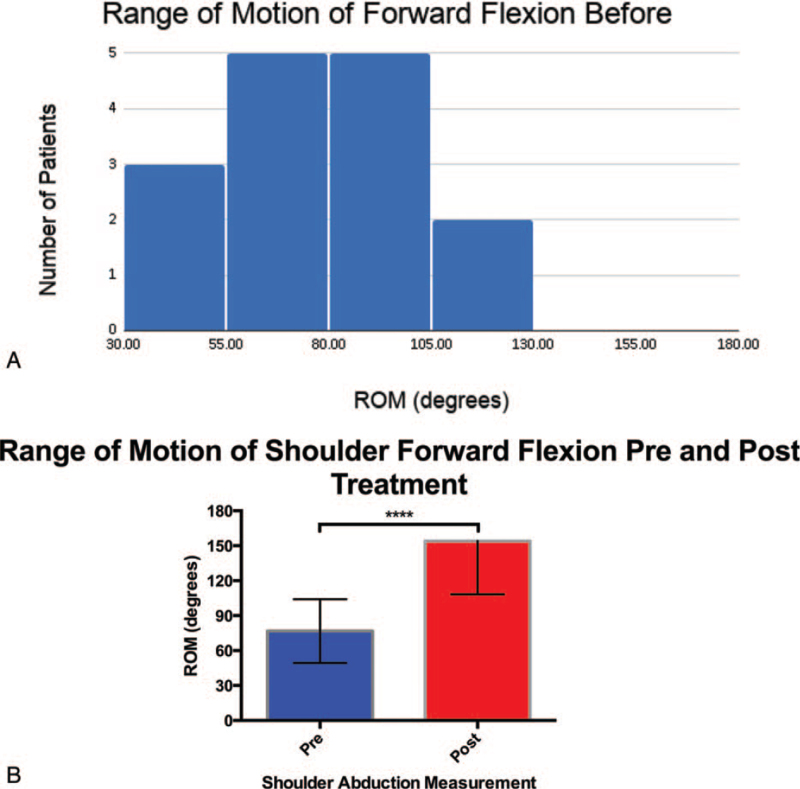
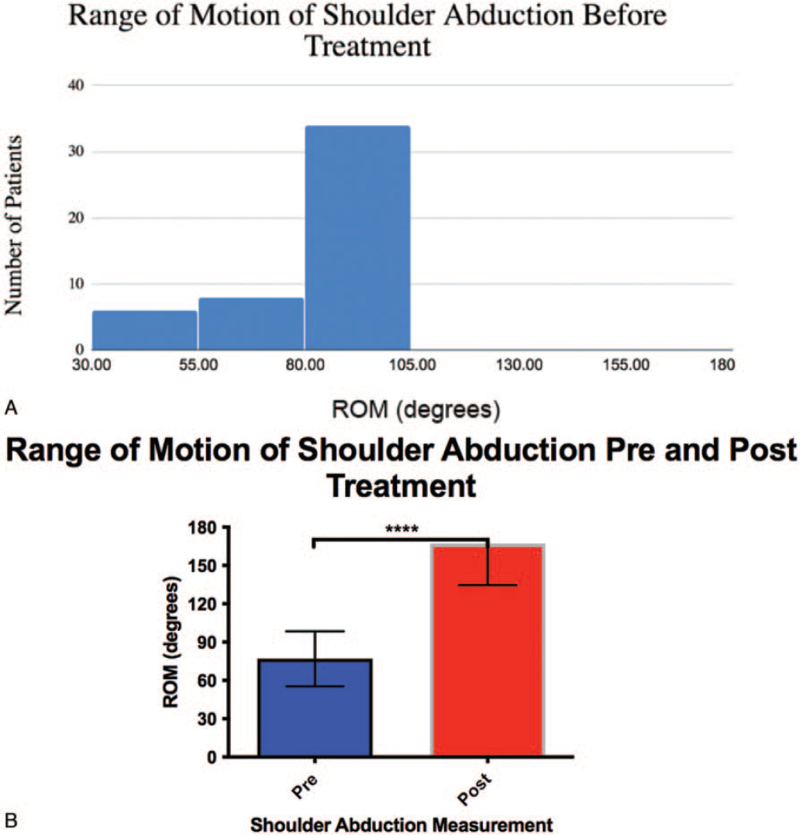
Currently, there is limited evidence to guide treatment and no standard management guidelines exist for treating frozen shoulder (FS). A general management approach consists of initial evaluation, range of motion (ROM) exercises, intra-articular injection of glucocorticoid, home exercise program (HEP), and/or physical therapies. However, the general approach lacks detail and has limited evidence of its effectiveness. This retrospective cohort study evaluates the short-term recovery of near-full to full-ROM technique followed by an instructed HEP for strengthening and coordinating shoulder girdle muscle group for FS management. This study details our experiences following a general approach to managing FS and aims to fill this knowledge void, providing additional context of the efficacy of FS management in the real-world. Seven-two adult patients with FS (46 females, 26 males; mean age of 66; standard deviation of 15.1; range 23-87) from an orthopedic and physical medicine and sport medicine office between 2014 and 2018 were included in this study. Following general management of FS, patients received a glucocorticoid-lidocaine mixture injection administered to the respective shoulder at the glenohumeral joint space and/or subacromial separately. Immediately, patients underwent active manipulation of the affected shoulder in 3 directions: forward flexion, abduction, and extension in the sagittal plane. Lastly, patients were instructed to perform movements similar to the active manipulation protocol as a HEP. The abduction and forward flexion ROM showed significant improvements with the described protocol. Following treatment, there was a 90.20° and 77.33° increase in average shoulder abduction and forward flexion ROM, respectively (P < .05). The immediate goal of this protocol was to gain maximum ROM in different directions of shoulder mobility. Following the general management of FS, active manipulation under local anesthetic was a highly effective treatment modality for adhesive capsulitis that was time-saving and cost-effective.
目前,针对冻结肩(FS)的治疗方法,仅有有限的证据可供参考,也没有标准的管理指南。一般的管理方法包括初始评估、关节活动度(ROM)练习、关节内注射糖皮质激素、家庭锻炼计划(HEP)和/或物理治疗。然而,这种常规方法缺乏细节,其有效性的证据也有限。本回顾性队列研究评估了在接近全关节活动度或全关节活动度的恢复后,采用强化和协调肩部肌肉群的指导性 HEP 进行治疗的短期效果,以此治疗 FS。本研究详细介绍了我们在 FS 常规治疗方法中的经验,并旨在填补这一知识空白,为现实世界中 FS 管理的疗效提供更多的背景信息。本研究纳入了 2014 年至 2018 年间,一家骨科和物理医学与运动医学诊所中 72 名 FS 成年患者(46 名女性,26 名男性;平均年龄 66 岁;标准差 15.1 岁;年龄范围 23-87 岁)。在对 FS 进行常规治疗后,患者分别在盂肱关节间隙和/或肩峰下接受糖皮质激素-利多卡因混合液注射。紧接着,患者接受了受累肩部的 3 个方向的主动关节活动度(ROM)练习:矢状面的前屈、外展和伸展。最后,患者被指导进行类似于主动关节活动度练习的HEP。描述的方案可显著改善外展和前屈 ROM。治疗后,患者的平均肩部外展和前屈 ROM 分别增加了 90.20°和 77.33°(P < .05)。该方案的直接目标是获得不同方向的最大肩部活动度。在 FS 的常规治疗后,在局部麻醉下进行主动关节活动度练习是一种针对粘连性肩关节囊炎的高效治疗方法,这种方法省时、经济。