Upper GI and HPB Surgery, Fondazione IRCCS Istituto Nazionale Tumori, Milan, Italy.
Department of Oncology and Hemato-Oncology, University of Milan, Milan, Italy.
Ann Surg Oncol. 2022 May;29(5):3096-3108. doi: 10.1245/s10434-021-11010-0. Epub 2022 Jan 1.
No consensus exists on the resection extent needed to ensure oncological safety in gastrectomy for gastric adenocarcinoma (GAC). This study aims to assess the impact of margin adequacy according to Japanese Gastric Cancer Association (JGCA) guidelines on overall survival (OS).
Patients who underwent surgery for stage I-III GAC at our institution between 2010 and 2017 were included. Margin adequacy according to JGCA, National Comprehensive Cancer Network (NCCN), and European Society for Medical Oncology (ESMO) guidelines was assessed, and their predictive value on OS was evaluated with Harrell's C-index. Patients were analyzed according to their margins' adherence to JGCA guidelines, and a propensity score matching (PSM) was run. Indication to either total gastrectomy (TG) or distal gastrectomy (DG) according to each guideline was also assessed.
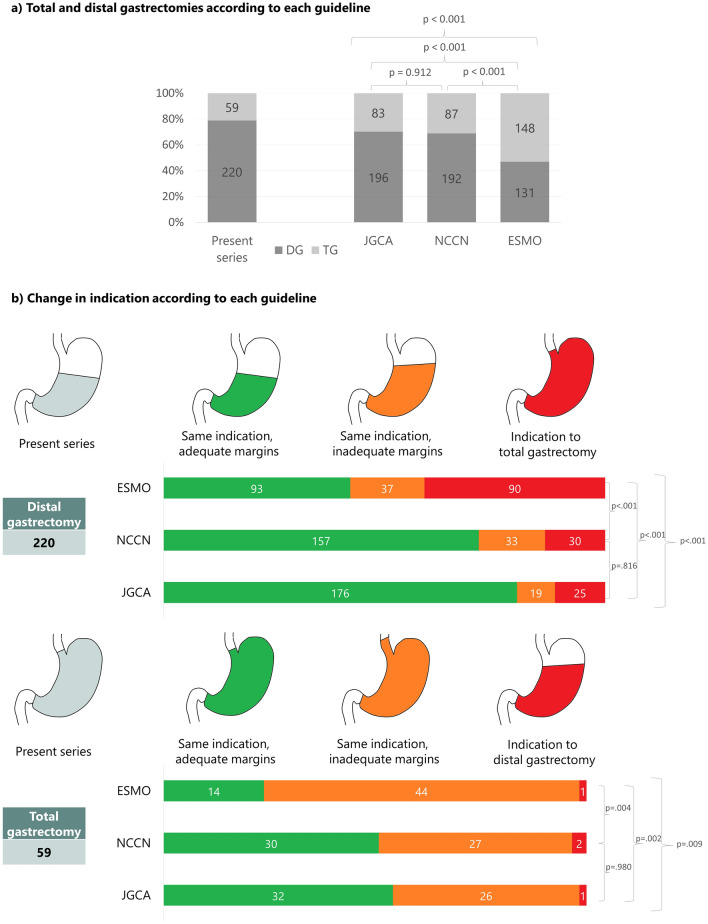
A total of 279 patients were included, of whom 220 (79%) underwent DG. Adequate margins according to JGCA were obtained in 209 patients (75%). On multivariate analysis, JGCA margin adequacy was independently associated with OS, together with American Society of Anesthesiologist class, neoadjuvant chemotherapy, lymphadenectomy extent, R0 resection, and postoperative N stage. After PSM, patients with JGCA adequate margins showed better OS, recurrence-free survival (RFS), and local RFS than patients with JGCA inadequate margins. For 220 DG, JGCA guidelines would have recommended TG in 25 patients (11%), NCCN in 30 (14%), and ESMO in 90 (41%) (p < 0.001).
Adequacy of surgical resection margins to JGCA guidelines leads to improved survival outcomes and allows for a more organ-preserving approach than Western guidelines.
在胃腺癌(GAC)的胃切除术时,对于确保肿瘤学安全性所需的切除范围尚未达成共识。本研究旨在评估根据日本胃癌协会(JGCA)指南判断切缘是否充分对总生存期(OS)的影响。
纳入了 2010 年至 2017 年期间在我院接受 I-III 期 GAC 手术的患者。根据 JGCA、美国国家综合癌症网络(NCCN)和欧洲肿瘤内科学会(ESMO)指南评估切缘是否充分,并使用 Harrell's C 指数评估其对 OS 的预测价值。根据患者切缘是否符合 JGCA 指南进行分析,并进行倾向评分匹配(PSM)。还评估了根据每个指南选择全胃切除术(TG)或胃远端切除术(DG)的适应证。
共纳入 279 例患者,其中 220 例(79%)行 DG。209 例(75%)患者获得了 JGCA 充分的切缘。多变量分析显示,JGCA 切缘充分与 OS 独立相关,与美国麻醉医师协会(ASA)分级、新辅助化疗、淋巴结清扫范围、R0 切除和术后 N 分期有关。PSM 后,JGCA 切缘充分的患者 OS、无复发生存(RFS)和局部 RFS 均优于 JGCA 切缘不充分的患者。对于 220 例行 DG 的患者,JGCA 指南建议行 TG 的患者有 25 例(11%),NCCN 指南有 30 例(14%),ESMO 指南有 90 例(41%)(p<0.001)。
根据 JGCA 指南判断切缘是否充分可改善生存结果,并可采用比西方指南更具保留器官的方法。