Adusumilli Gautam, Pederson John M, Hardy Nicole, Kallmes Kevin M, Hutchison Kristen, Kobeissi Hassan, Heiferman Daniel M, Heit Jeremy J
Department of Radiology and Neurosurgery, Stanford University, Stanford, CA, United States.
Nested Knowledge, Inc, St. Paul, MN, United States.
Front Neurol. 2021 Dec 17;12:759759. doi: 10.3389/fneur.2021.759759. eCollection 2021.
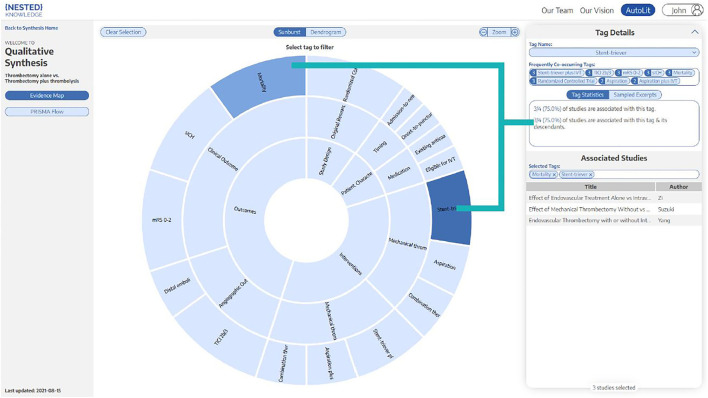
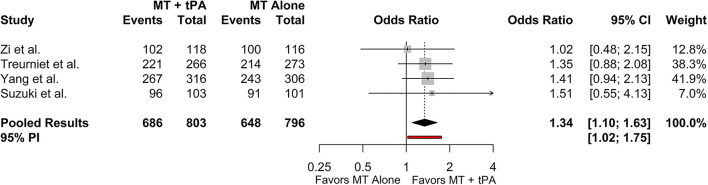
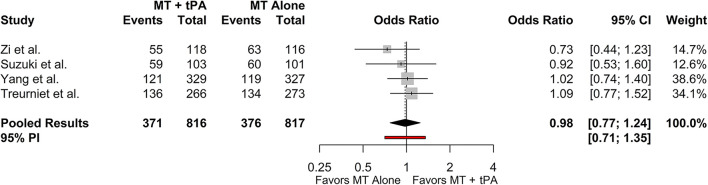
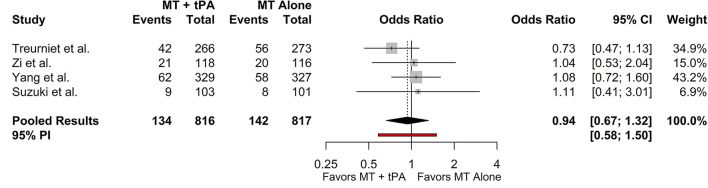
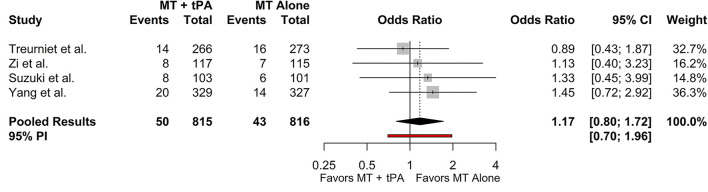
Mechanical thrombectomy (MT) is now the standard-of-care treatment for acute ischemic stroke (AIS) of the anterior circulation and may be performed irrespective of intravenous tissue plasminogen activator (IV-tPA) eligibility prior to the procedure. This study aims to understand better if tPA leads to higher rates of reperfusion and improves functional outcomes in AIS patients after MT and to simultaneously evaluate the functionality and efficiency of a novel semi-automated systematic review platform. The Nested Knowledge AutoLit semi-automated systematic review platform was utilized to identify randomized control trials published between 2010 and 2021 reporting the use of mechanical thrombectomy and IV-tPA (MT+tPA) vs. MT alone for AIS treatment. The primary outcome was the rate of successful recanalization, defined as thrombolysis in cerebral infarction (TICI) scores ≥2b. Secondary outcomes included 90-day modified Rankin Scale (mRS) 0-2, 90-day mortality, distal embolization to new territory, and symptomatic intracranial hemorrhage (sICH). A separate random effects model was fit for each outcome measure. We subjectively found Nested Knowledge to be highly streamlined and effective at sourcing the correct literature. Four studies with 1,633 patients, 816 in the MT+tPA arm and 817 in the MT arm, were included in the meta-analysis. In each study, patient populations consisted of only tPA-eligible patients and all imaging and clinical outcomes were adjudicated by an independent and blinded core laboratory. Compared to MT alone, patients treated with MT+tPA had higher odds of eTICI ≥2b (OR = 1.34 [95% CI: 1.10; 1.63]). However, there were no statistically significant differences in the rates of 90-day mRS 0-2 (OR = 0.98 [95% CI: 0.77; 1.24]), 90-day mortality (OR = 0.94 [95% CI: 0.67; 1.32]), distal emboli (OR = 0.94 [95% CI: 0.25; 3.60]), or sICH (OR = 1.17 [95% CI: 0.80; 1.72]). Administering tPA prior to MT may improve the rates of recanalization compared to MT alone in tPA-eligible patients being treated for AIS, but a corresponding improvement in functional and safety outcomes was not present in this review. Further studies looking at the role of tPA before mechanical thrombectomy in different cohorts of patients could better clarify the role of tPA in the treatment protocol for AIS.
机械取栓术(MT)目前是前循环急性缺血性卒中(AIS)的标准治疗方法,且在手术前无论是否符合静脉注射组织纤溶酶原激活剂(IV-tPA)的条件均可进行。本研究旨在更好地了解tPA是否能提高AIS患者在MT术后的再灌注率并改善功能结局,同时评估一个新型半自动系统评价平台的功能和效率。利用嵌套知识自动文献半自动系统评价平台来识别2010年至2021年间发表的随机对照试验,这些试验报告了使用机械取栓术联合IV-tPA(MT+tPA)与单纯MT治疗AIS的情况。主要结局是成功再通率,定义为脑梗死溶栓(TICI)评分≥2b。次要结局包括90天改良Rankin量表(mRS)评分为0-2、90天死亡率、新区域的远端栓塞和症状性颅内出血(sICH)。对每个结局指标分别拟合一个随机效应模型。我们主观认为嵌套知识在获取正确文献方面高度精简且有效。荟萃分析纳入了四项研究,共1633例患者,MT+tPA组816例,MT组817例。在每项研究中,患者群体仅包括符合tPA条件的患者,所有影像学和临床结局均由一个独立且盲法的核心实验室判定。与单纯MT相比,接受MT+tPA治疗的患者eTICI≥2b的几率更高(OR = 1.34 [95% CI:1.10;1.63])。然而,在90天mRS评分为0-2的发生率(OR = 0.98 [95% CI:0.77;1.24])、90天死亡率(OR = 0.94 [95% CI:0.67;1.32])、远端栓子(OR = 0.94 [95% CI:0.25;3.60])或sICH(OR = 1.17 [95% CI:0.80;1.72])方面,没有统计学上的显著差异。与单纯MT相比,在接受AIS治疗的符合tPA条件的患者中,术前给予tPA可能会提高再通率,但本综述中未发现功能和安全性结局有相应改善。进一步研究tPA在不同患者群体的机械取栓术前的作用,可能会更好地阐明tPA在AIS治疗方案中的作用。