Division of Pulmonary and Critical Care Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
Clin Infect Dis. 2022 Sep 14;75(5):743-752. doi: 10.1093/cid/ciac003.
Systemic drug reaction (SDR) is a major safety concern with weekly rifapentine plus isoniazid for 12 doses (3HP) for latent tuberculosis infection (LTBI). Identifying SDR predictors and at-risk participants before treatment can improve cost-effectiveness of the LTBI program.
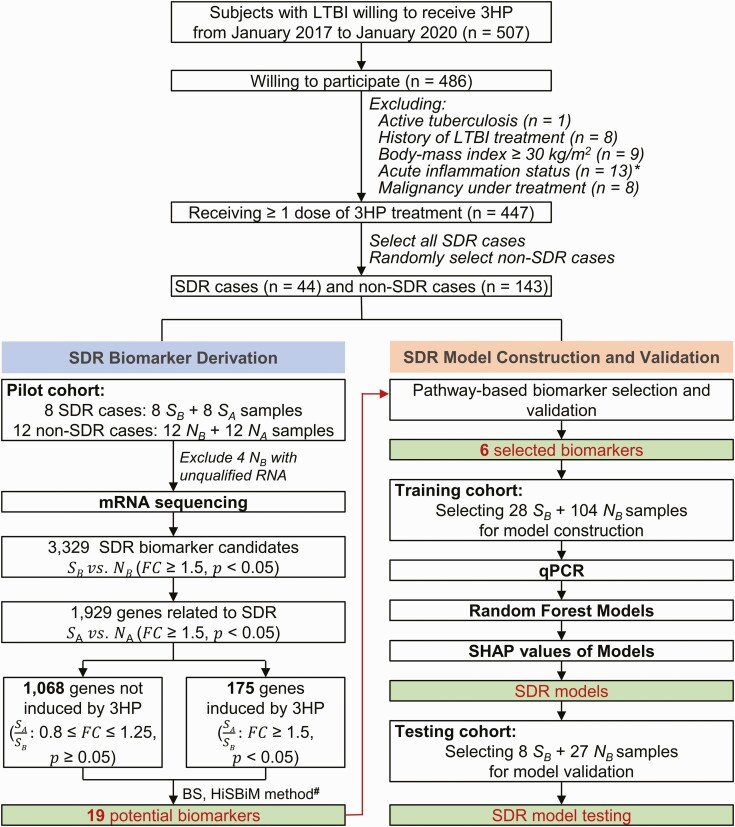
We prospectively recruited 187 cases receiving 3HP (44 SDRs and 143 non-SDRs). A pilot cohort (8 SDRs and 12 non-SDRs) was selected for generating whole-blood transcriptomic data. By incorporating the hierarchical system biology model and therapy-biomarker pathway approach, candidate genes were selected and evaluated using reverse-transcription quantitative polymerase chain reaction (RT-qPCR). Then, interpretable machine learning models presenting as SHapley Additive exPlanations (SHAP) values were applied for SDR risk prediction. Finally, an independent cohort was used to evaluate the performance of these predictive models.
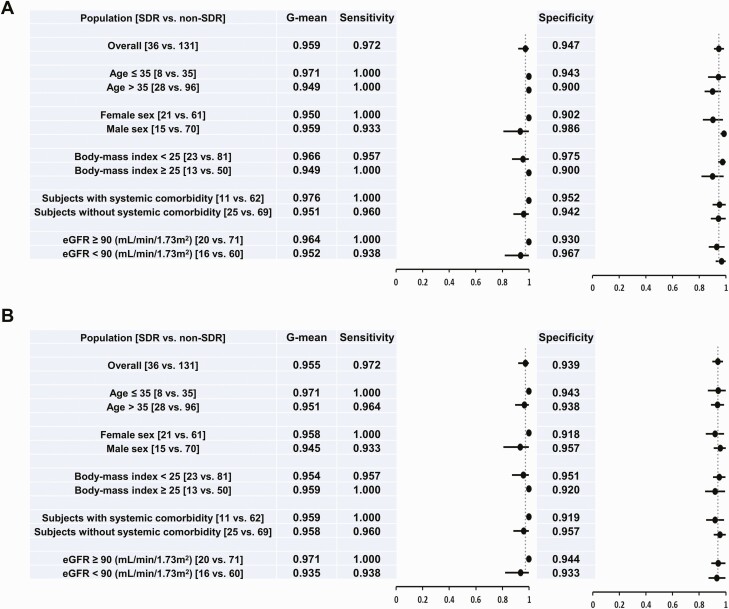
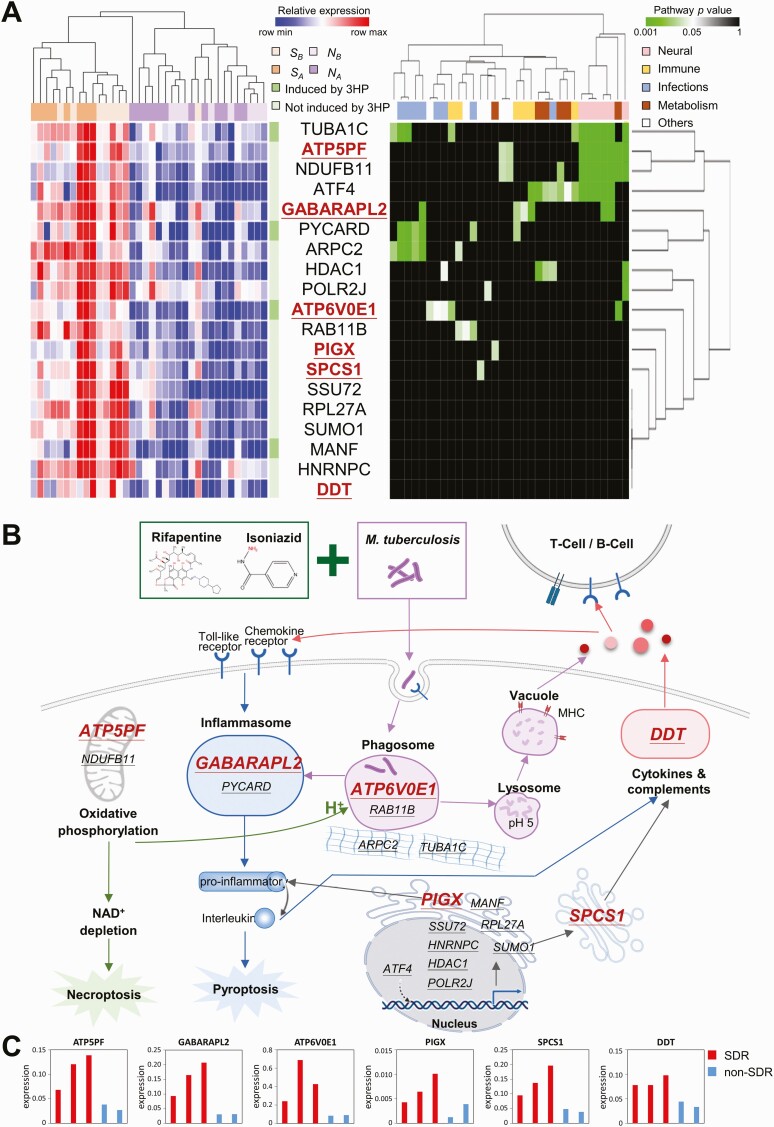
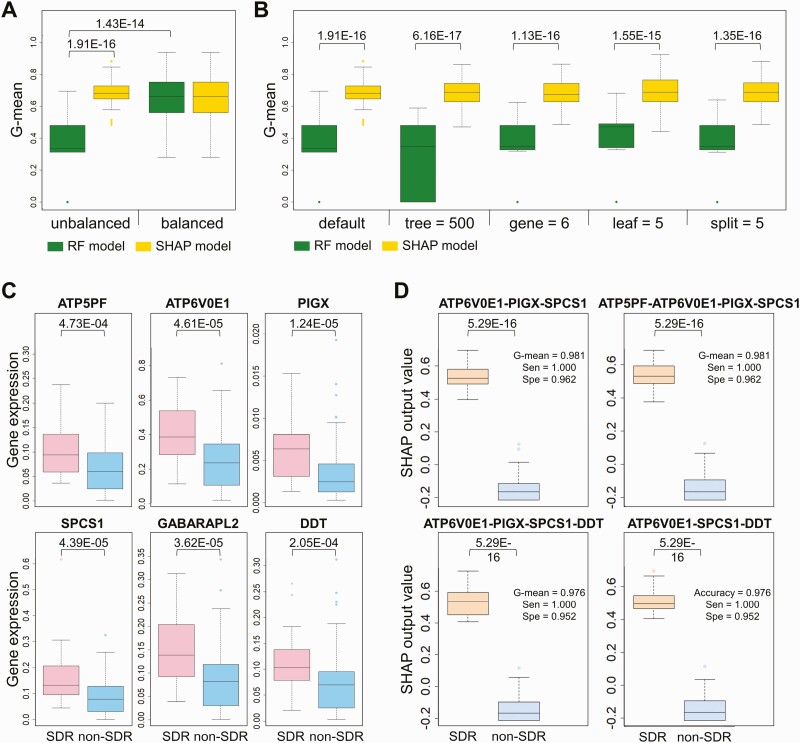
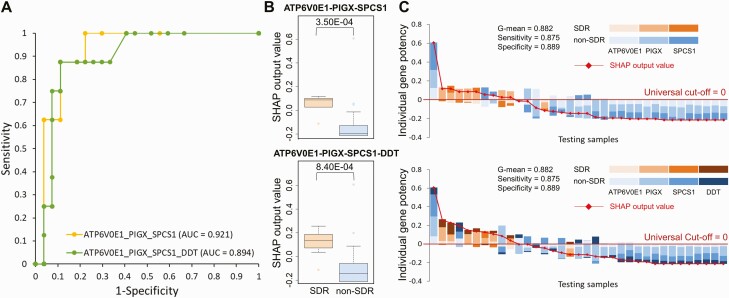
Based on the whole-blood transcriptomic profile of the pilot cohort and the RT-qPCR results of 2 SDR and 3 non-SDR samples in the training cohort, 6 genes were selected. According to SHAP values for model construction and validation, a 3-gene model for SDR risk prediction achieved a sensitivity and specificity of 0.972 and 0.947, respectively, under a universal cutoff value for the joint of the training (28 SDRs and 104 non-SDRs) and testing (8 SDRs and 27 non-SDRs) cohorts. It also worked well across different subgroups.
The prediction model for 3HP-related SDRs serves as a guide for establishing a safe and personalized regimen to foster the implementation of an LTBI program. Additionally, it provides a potential translational value for future studies on drug-related hypersensitivity.
每周利福喷丁加异烟肼治疗 12 剂(3HP)治疗潜伏性结核感染(LTBI)存在全身性药物反应(SDR)的重大安全隐患。在治疗前识别 SDR 预测因子和高危参与者可以提高 LTBI 计划的成本效益。
我们前瞻性招募了 187 例接受 3HP(44 例 SDR 和 143 例非 SDR)的患者。选择了一个试点队列(8 例 SDR 和 12 例非 SDR)生成全血转录组数据。通过纳入分层系统生物学模型和治疗生物标志物途径方法,选择候选基因并使用逆转录定量聚合酶链反应(RT-qPCR)进行评估。然后,应用可解释的机器学习模型(表现为 SHapley Additive exPlanations(SHAP)值)进行 SDR 风险预测。最后,使用独立队列评估这些预测模型的性能。
基于试点队列的全血转录组谱和训练队列中 2 例 SDR 和 3 例非 SDR 样本的 RT-qPCR 结果,选择了 6 个基因。根据模型构建和验证的 SHAP 值,在训练(28 例 SDR 和 104 例非 SDR)和测试(8 例 SDR 和 27 例非 SDR)队列的联合通用截止值下,SDR 风险预测的 3 基因模型的敏感性和特异性分别为 0.972 和 0.947。它在不同的亚组中也表现良好。
3HP 相关 SDR 的预测模型可作为制定安全个性化方案的指南,以促进 LTBI 计划的实施。此外,它为未来药物相关超敏反应的研究提供了潜在的转化价值。