Boston University School of Public Health, Boston, the Massachusetts Department of Public Health, Boston, Evalogic Services, Inc, Newton, the Tufts University School of Medicine, Boston, and the Department of Biostatistics, Harvard T. H. Chan School of Public Health, Boston, Massachusetts; and the Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California, San Diego, San Diego, California.
Obstet Gynecol. 2022 Feb 1;139(2):165-171. doi: 10.1097/AOG.0000000000004641.
To assess whether application of a standard algorithm to hospitalizations in the prenatal and postpartum (42 days) periods increases identification of severe maternal morbidity (SMM) beyond analysis of only the delivery event.
We performed a retrospective cohort study using data from the PELL (Pregnancy to Early Life Longitudinal) database, a Massachusetts population-based data system that links records from birth certificates to delivery hospital discharge records and nonbirth hospital records for all birthing individuals. We included deliveries from January 1, 2009, to December 31, 2018, distinguishing between International Classification of Diseases Ninth (ICD-9) and Tenth Revision (ICD-10) coding. We applied the modified Centers for Disease Control and Prevention algorithm for SMM used by the Alliance for Innovation on Maternal Health to hospitalizations across the antenatal period through 42 days postpartum. Morbidity was examined both with and without blood transfusion.
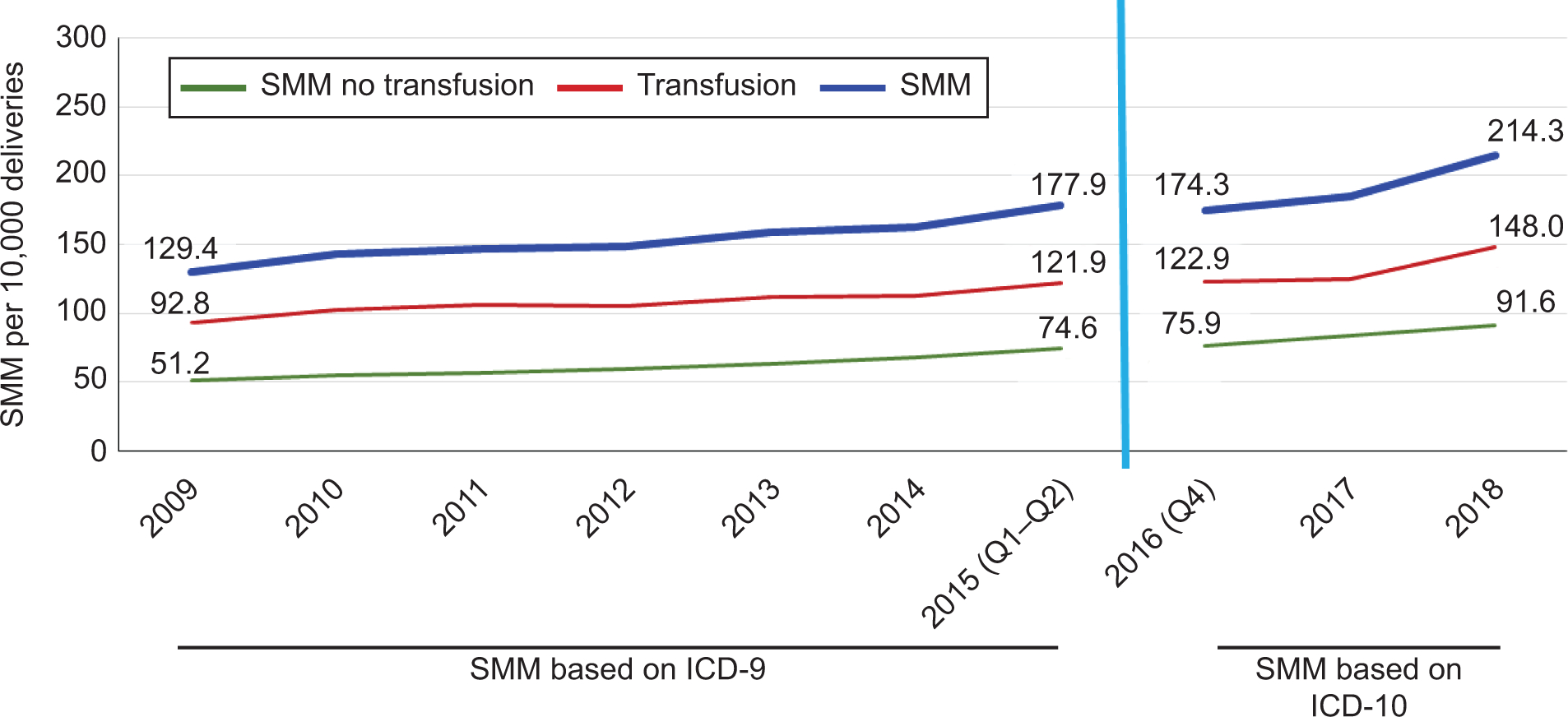
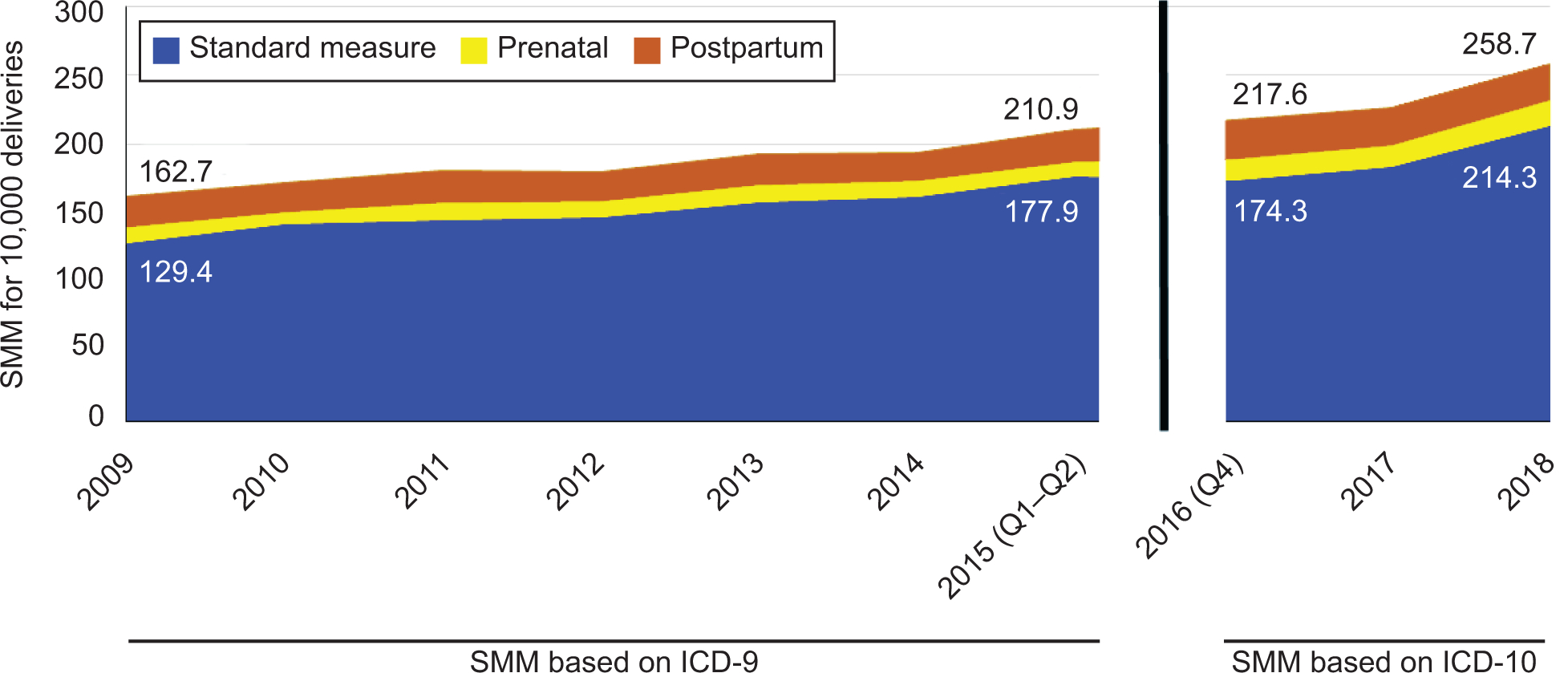
Overall, 594,056 deliveries were included in the analysis, and 3,947 deliveries met criteria for SMM at delivery without transfusion and 9,593 with transfusion for aggregate rates of 150.1 (95% CI 146.7-153.5) using ICD-9 codes and 196.6 (95% CI 189.5-203.7) using ICD-10 codes per 10,000 deliveries. Severe maternal morbidity at birth increased steadily across both ICD-9 and ICD-10 from 129.4 in 2009 (95% CI 126.2-132.6) using ICD-9 to 214.3 per 10,000 (95% CI 206.9-221.8) in 2018 using ICD-10. Adding prenatal and postpartum hospitalizations increased cases by 21.9% under both ICD-9 and ICD-10, resulting in a 2018 rate of 258.7 per 10,000 (95% CI 250.5-266.9). The largest increase in detected morbidity in the prenatal or postpartum time period was attributed to sepsis cases.
Inclusion of prenatal and postpartum hospitalizations in the identification of SMM resulted in increased ascertainment of morbid events. These results suggest a need to ensure surveillance of care quality activities beyond the birth event.
评估在产前和产后(42 天)期间应用标准算法是否可以增加严重产妇发病率(SMM)的识别率,而不仅仅局限于分娩事件的分析。
我们使用来自 PELL(妊娠至早期生命纵向)数据库的回顾性队列研究数据,该数据库是一个马萨诸塞州人群为基础的数据系统,可将出生证明记录与分娩医院出院记录以及所有分娩个体的非分娩医院记录相链接。我们纳入了 2009 年 1 月 1 日至 2018 年 12 月 31 日的分娩记录,分别使用国际疾病分类第 9 版(ICD-9)和第 10 版(ICD-10)编码进行区分。我们应用了由母婴健康创新联盟使用的改良疾病控制和预防中心 SMM 算法,用于产前至产后 42 天的住院治疗。无论是否输血,我们都使用了该算法来检查发病率。
总体而言,共有 594056 次分娩纳入分析,其中有 3947 次分娩在无输血时符合 SMM 标准,有 9593 次分娩在输血时符合标准,总体 SMM 发生率为每 10000 次分娩 150.1(95%CI 146.7-153.5),使用 ICD-9 编码;为 196.6(95%CI 189.5-203.7),使用 ICD-10 编码。在使用 ICD-9 时,2009 年分娩时的严重产妇发病率从 129.4(95%CI 126.2-132.6)稳步上升至 2018 年的每 10000 次分娩 214.3(95%CI 206.9-221.8),而在使用 ICD-10 时则为每 10000 次分娩 214.3(95%CI 206.9-221.8)。在这两种编码系统下,产前和产后住院治疗的增加都使病例增加了 21.9%,导致 2018 年的发病率为每 10000 次分娩 258.7(95%CI 250.5-266.9)。在产前或产后时期发现的发病率增加最大的原因是败血症病例。
在 SMM 的识别中纳入产前和产后住院治疗会增加对不良事件的检出率。这些结果表明,需要确保在分娩事件之外对护理质量活动进行监测。