Department of Orthopedic Surgery, Seoul National University Hospital, 101 Daehak-no, Jongno-gu, Seoul, South Korea.
Department of Orthopedic Surgery, SNU Seoul Hospital, Seoul, South Korea.
J Foot Ankle Res. 2022 Jan 6;15(1):1. doi: 10.1186/s13047-021-00508-1.
Multi-segment foot models (MFMs) for assessing three-dimensional segmental foot motions are calculated via various analytical methods. Although validation studies have already been conducted, we cannot compare their results because the experimental environments in previous studies were different from each other. This study aims to compare the kinematics, repeatability, and reproducibility of five MFMs in the same experimental conditions.
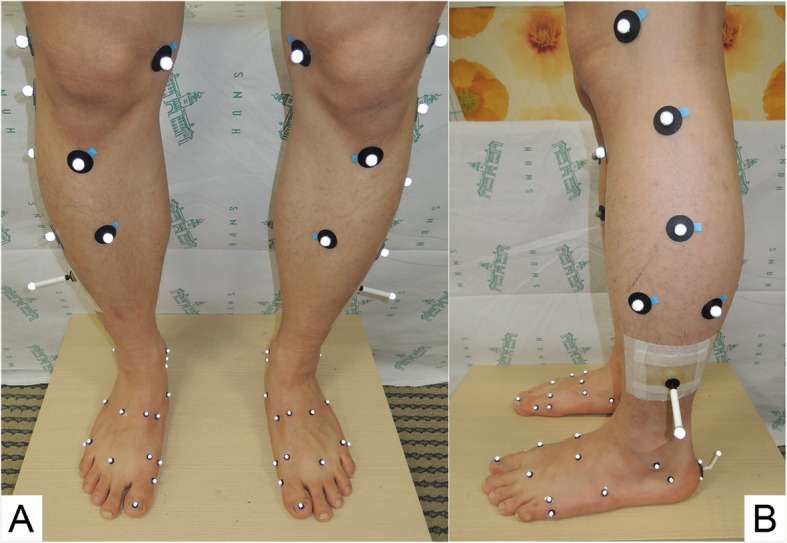
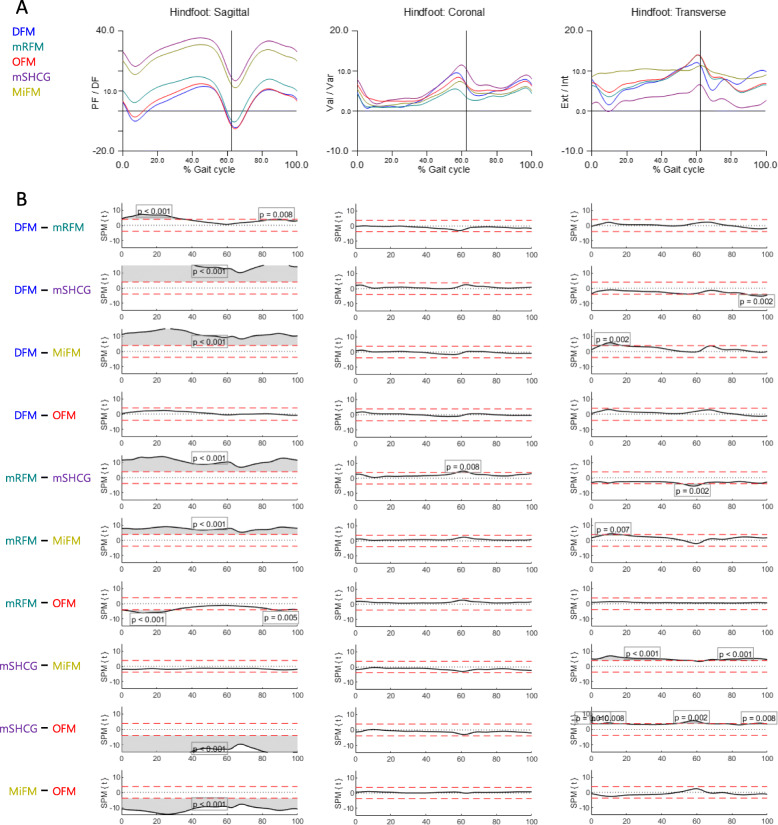
Eleven healthy males with a mean age of 26.5 years participated in this study. We created a merged 29-marker set including five MFMs: Oxford (OFM), modified Rizzoli (mRFM), DuPont (DFM), Milwaukee (MiFM), and modified Shriners Hospital for Children Greenville (mSHCG). Two operators applied the merged model to participants twice, and then we analysed two relative angles of three segments: shank-hindfoot (HF) and hindfoot-forefoot (FF). Coefficients of multiple correlation (CMC) and mean standard errors were used to assess repeatability and reproducibility, and statistical parametric mapping (SPM) of the t-value was employed to compare kinematics.
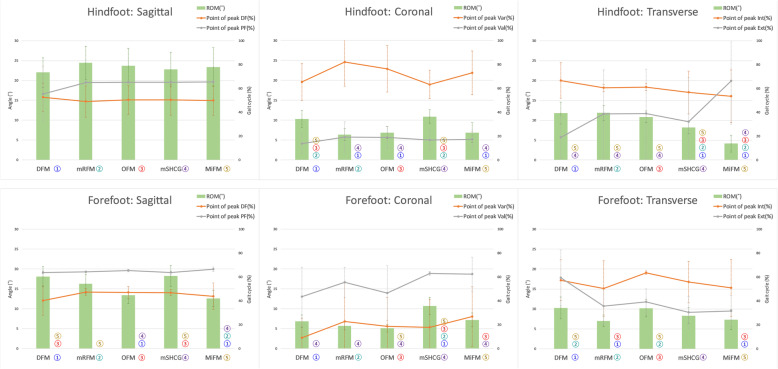
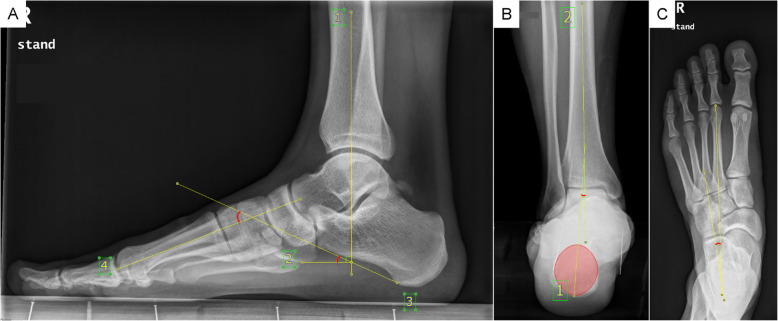
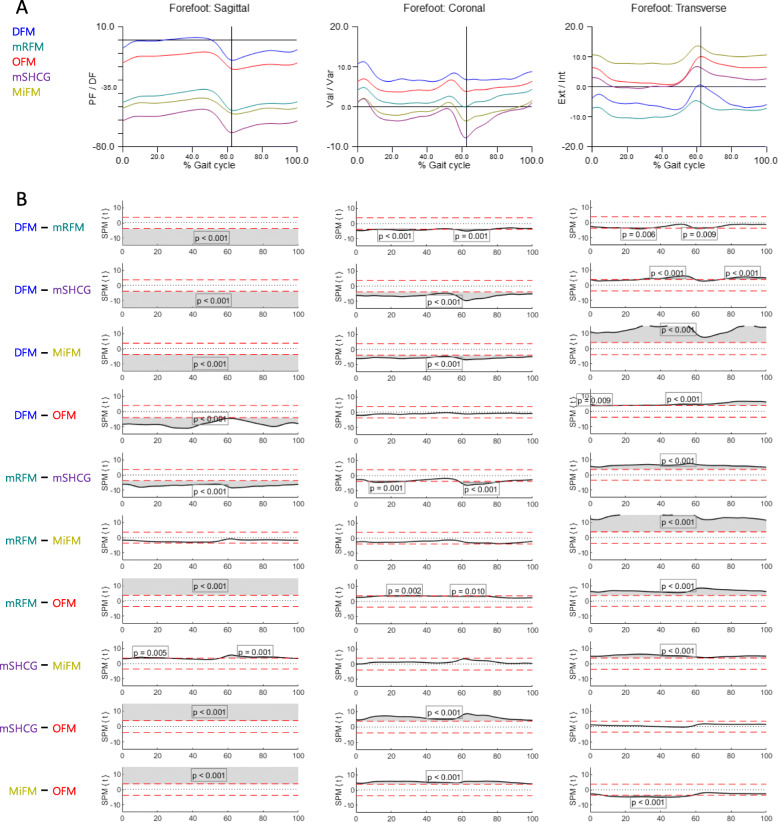
HF varus/valgus of the MiFM and mSHCG models, which rotated the segment according to radiographic or goniometric measurements during the reference frame construction, were significantly more repeatable and reproducible, compared to other models. They showed significantly more dorsiflexed HF and plantarflexed FF due to their static offset angles. DFM and mSHCG showed a greater range of motion (ROM), and some models had significantly different FF points of peak angle.
Under the same conditions, rotating the segment according to the appropriate offset angle obtained from radiographic or goniometric measurement increased reliability, but all MFMs had clinically acceptable reliability compared to previous studies. Moreover, in some models, especially HF varus/valgus, there were differences in ROM and points of peak angle even with no statistical difference in SPM curves. Therefore, based on the results of this study, clinicians and researchers involved in the evaluation of foot and ankle dysfunction need an understanding of the specific features of each MFM to make accurate decisions.
多节段足模型(MFMs)用于评估三维节段性足运动,通过各种分析方法进行计算。尽管已经进行了验证研究,但我们无法比较它们的结果,因为之前研究中的实验环境彼此不同。本研究旨在比较五种 MFMs 在相同实验条件下的运动学、可重复性和再现性。
11 名平均年龄为 26.5 岁的健康男性参与了这项研究。我们创建了一个合并的 29 个标记集,包括五个 MFMs:牛津(OFM)、改良里兹利(mRFM)、杜邦(DFM)、密尔沃基(MiFM)和改良 Shriners 儿童医院格林维尔(mSHCG)。两名操作员两次将合并模型应用于参与者,然后我们分析了三个节段的两个相对角度:小腿-后足(HF)和后足-前足(FF)。使用多重相关系数(CMC)和平均标准误差评估可重复性和再现性,并使用 t 值的统计参数映射(SPM)比较运动学。
MiFM 和 mSHCG 模型的 HF 内翻/外翻,这些模型在参考框架构建期间根据放射照相或角度测量旋转节段,与其他模型相比,具有更高的可重复性和再现性。由于其静态偏置角度,它们的 HF 表现出更明显的背屈和 FF 的跖屈。DFM 和 mSHCG 显示出更大的运动范围(ROM),并且一些模型的 FF 峰值角度点有明显差异。
在相同条件下,根据从放射照相或角度测量获得的适当偏置角度旋转节段会提高可靠性,但与之前的研究相比,所有 MFMs 都具有可接受的临床可靠性。此外,在一些模型中,特别是 HF 内翻/外翻,即使 SPM 曲线没有统计学差异,ROM 和峰值角度点也存在差异。因此,基于这项研究的结果,涉及足踝功能评估的临床医生和研究人员需要了解每个 MFM 的特定特征,以便做出准确的决策。