Kandhari Navneet, Khoury Shafik, Behr Elijah R, Miles Chris
St Georges University Hospital NHS Foundation Trust, Blackshaw Road, Tooting, London SW17 0QT, UK.
Cardiovascular Clinical Academic Group, Molecular and Clinical Sciences Institute, St George's University of London, Cranmer Terrace, Tooting, London SW17 0RE, UK.
Eur Heart J Case Rep. 2021 Nov 22;5(11):ytab422. doi: 10.1093/ehjcr/ytab422. eCollection 2021 Nov.
Arrhythmogenic left ventricular cardiomyopathy (ALVC) is a rare form of arrhythmogenic cardiomyopathy characterized by fibrofatty replacement of left ventricular myocardium, malignant arrhythmia, and sudden cardiac death. The definition incorporates several genetic causes, including pathogenic variation in the Filamin C gene (FLNC). Although awareness of ALVC has improved, identification remains challenging and diagnostic criteria continue to evolve.
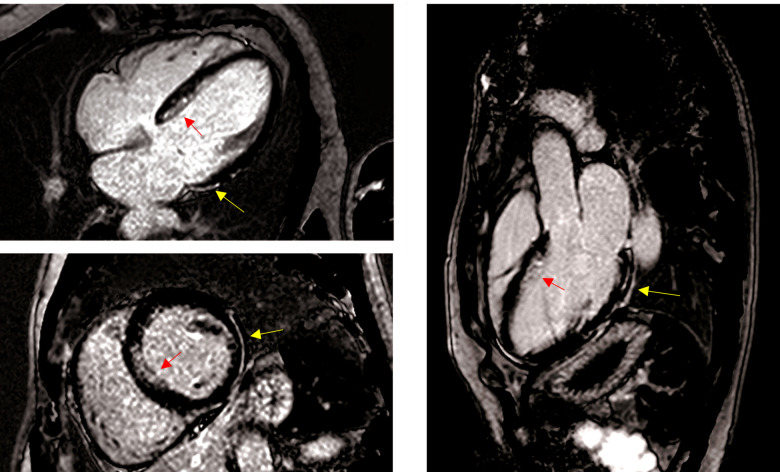
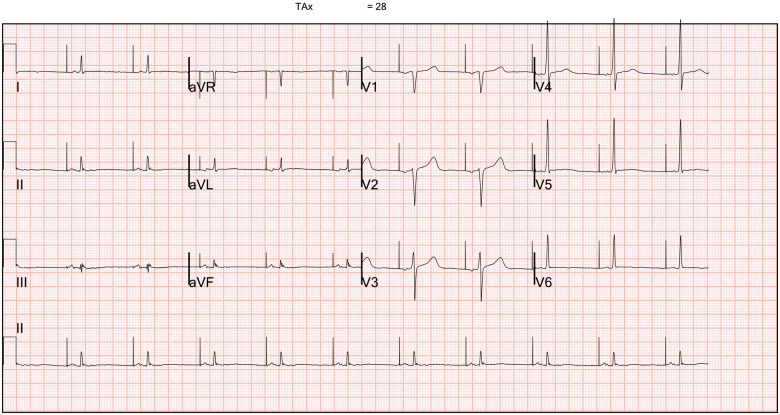
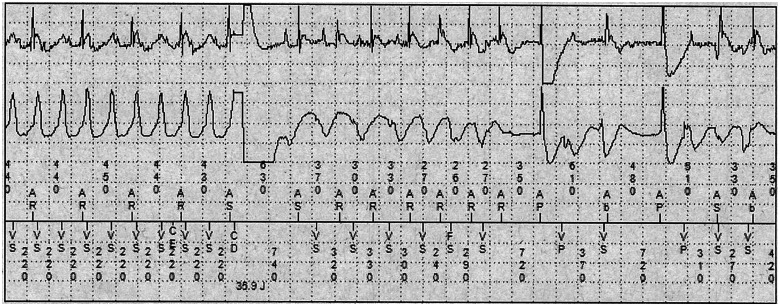
A 50-year-old athletic male was admitted following an out-of-hospital cardiac arrest due to ventricular tachycardia (VT) whilst playing football. Coronary angiography revealed unobstructed epicardial vessels and the diagnosis of ALVC was suggested by cardiovascular magnetic resonance imaging, which demonstrated a mildly dilated and moderately impaired left ventricle with epicardial late gadolinium enhancement in the basal to mid-lateral walls and subendocardial septum. Initial testing with a cardiomyopathy and arrhythmia gene panel was negative but extended testing uncovered a likely pathogenic variant in FLNC. Subsequently, the patient experienced a recurrence of sustained VT necessitating implantable cardioverter-defibrillator (ICD) therapies, ultimately undergoing a combined epicardial and endocardial VT ablation 4 years after presentation. Six months post-ablation, he was asymptomatic and his arrhythmia rendered quiescent.
Arrhythmogenic cardiomyopathy should be considered in the evaluation of an initially unexplained cardiac arrest. This case characterizes the clinical features of a patient with FLNC cardiomyopathy and emphasizes the utility of genetic testing using modern gene panels in patients with comparable phenotypes. We also demonstrate that optimal medical therapy with antiarrhythmic drugs, exercise restriction, ICD insertion, and catheter ablation can be useful in the management of ALVC with positive outcomes.
致心律失常性左室心肌病(ALVC)是致心律失常性心肌病的一种罕见形式,其特征为左室心肌纤维脂肪组织替代、恶性心律失常和心源性猝死。该定义包含多种遗传病因,包括细丝蛋白C基因(FLNC)的致病性变异。尽管对ALVC的认识有所提高,但诊断仍具有挑战性,诊断标准也在不断演变。
一名50岁的男性运动员在踢足球时因室性心动过速(VT)发生院外心脏骤停后入院。冠状动脉造影显示心外膜血管无阻塞,心血管磁共振成像提示ALVC诊断,该检查显示左心室轻度扩张、中度功能受损,心外膜下基底至中外侧壁及心内膜下间隔延迟钆增强。最初的心肌病和心律失常基因检测结果为阴性,但进一步检测发现FLNC存在可能的致病变异。随后,患者持续性VT复发,需要植入式心律转复除颤器(ICD)治疗,最终在就诊4年后接受了心外膜和心内膜联合VT消融术。消融术后6个月,他无症状,心律失常得到控制。
在评估最初原因不明的心脏骤停时应考虑致心律失常性心肌病。本病例描述了FLNC心肌病患者的临床特征,并强调了在具有类似表型的患者中使用现代基因检测板进行基因检测的实用性。我们还证明,使用抗心律失常药物、限制运动、植入ICD和导管消融等最佳药物治疗对ALVC的管理可能有用且效果良好。