Department of Radiology, University of California, San Francisco, San Francisco, CA, USA.
Department of Radiology, Urology, and Radiation Oncology, University of Washington, Seattle, WA, USA.
Abdom Radiol (NY). 2022 Mar;47(3):1133-1141. doi: 10.1007/s00261-021-03389-x. Epub 2022 Jan 7.
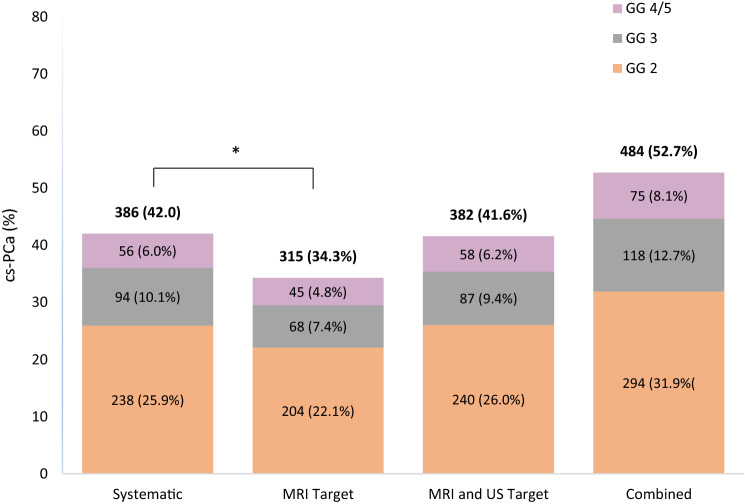
To identify predictors of when systematic biopsy leads to a higher overall prostate cancer grade compared to targeted biopsy.
918 consecutive patients who underwent prostate MRI followed by MRI/US fusion biopsy and systematic biopsies from January 2015 to November 2019 at a single academic medical center were retrospectively identified. The outcome was upgrade of PCa by systematic biopsy, defined as cases when systematic biopsy led to a Gleason Grade (GG) ≥ 2 and greater than the maximum GG detected by targeted biopsy. Generalized linear regression and conditional logistic regression were used to analyze predictors of upgrade.
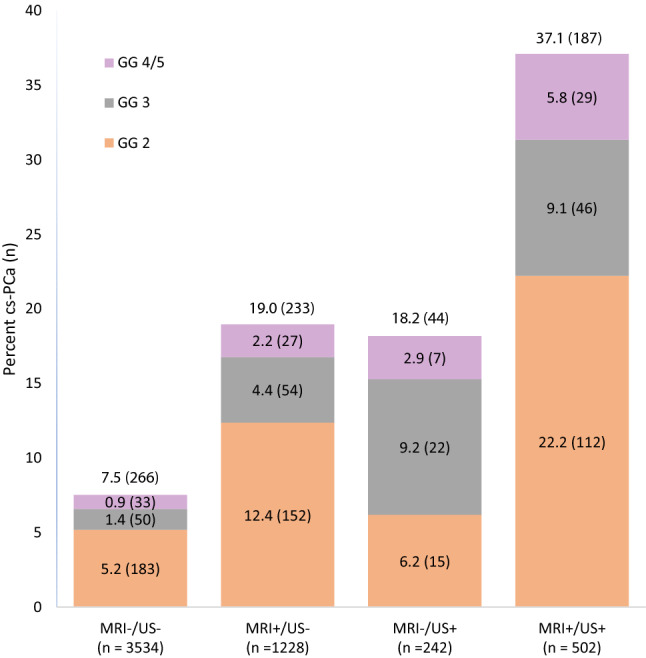
At the gland level, the presence of an US-visible lesion was associated with decreased upgrade (OR 0.64, 95% CI 0.44-0.93, p = 0.02). At the sextant level, upgrade was more likely to occur through the biopsy of sextants with MRI-visible lesions (OR 2.58, 95% CI 1.87-3.63, p < 0.001), US-visible lesions (OR 1.83, 95% CI 1.14-2.93, p = 0.01), and ipsilateral lesions (OR 3.89, 95% CI 2.36-6.42, p < 0.001).
Systematic biopsy is less valuable in patients with an US-visible lesion, and more likely to detect upgrades in sextants with imaging abnormalities. An approach that takes additional samples from regions with imaging abnormalities may provide analogous information to systematic biopsy.
确定系统活检与靶向活检相比导致前列腺癌整体分级升高的预测因素。
回顾性分析了 2015 年 1 月至 2019 年 11 月在一家学术医疗中心接受前列腺 MRI 检查、MRI/US 融合活检和系统活检的 918 例连续患者。主要结局为系统活检导致前列腺癌升级,定义为系统活检导致 Gleason 分级(GG)≥2 且高于靶向活检检测到的最大 GG。采用广义线性回归和条件逻辑回归分析预测升级的因素。
在腺体水平上,US 可见病变的存在与升级降低相关(OR 0.64,95%CI 0.44-0.93,p=0.02)。在六区分区水平上,通过活检 MRI 可见病变(OR 2.58,95%CI 1.87-3.63,p<0.001)、US 可见病变(OR 1.83,95%CI 1.14-2.93,p=0.01)和同侧病变(OR 3.89,95%CI 2.36-6.42,p<0.001)的六分区发生升级的可能性更大。
在 US 可见病变患者中,系统活检的价值较低,而在影像学异常的六分区中更有可能检测到升级。从影像学异常的区域采集额外样本的方法可能提供与系统活检类似的信息。