Department of Neurology, Medical Faculty, Heinrich-Heine-University Düsseldorf, Moorenstraße 5, 40225, Düsseldorf, Germany.
LWL-Clinics Muenster, Muenster, Germany.
J Neurol. 2022 May;269(5):2806-2818. doi: 10.1007/s00415-021-10956-1. Epub 2022 Jan 9.
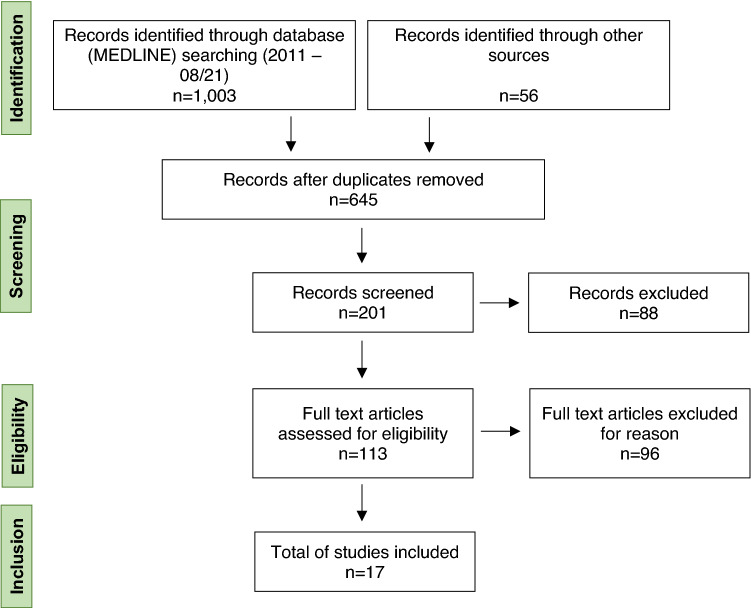
A critical issue in the management of relapsing MS (RMS) is the discontinuation of disease-modifying treatments (DMT) due to lack of efficacy, intolerability or impending risks. With new therapeutic agents introduced into the treatment of RMS, immediate- and long-term consequences of sequential drug use, as well as the effect of the sequence in which the drugs are given, are unclear but may affect efficacy, adverse events, and long-term immunocompetence. In the absence of clinical studies specifically addressing these concerns, observations from clinical practice are of particular value in guiding current management algorithms. Prompted by a study published by Ferraro et al. in this journal, we set out to provide an overview of the published real-world evidence on the effectiveness and safety of switching from fingolimod to another DMT in patients with active RMS. Seventeen publications reporting relevant information were identified. The literature suggests that immune cell depletion induced by alemtuzumab or ocrelizumab is associated with an increased risk of relapse and worsening disability in patients switching from fingolimod compared to patients switching from other therapeutic agents. However, the evidence reported for natalizumab and cladribine is inconclusive. While shortening of the washout period may limit early disease reactivation after fingolimod discontinuation, there is no strong evidence that the duration of the washout period or the absolute lymphocyte count at baseline are predictors of attenuated long-term efficacy. Further real-world studies are required to better understand outcomes among patients who are under-represented in controlled trials.
在复发性多发性硬化症(RMS)的管理中,一个关键问题是由于疗效不佳、不耐受或即将出现风险而停止使用疾病修正治疗(DMT)。随着新的治疗药物被引入 RMS 的治疗中,连续使用药物的即时和长期后果,以及药物给予的顺序的影响尚不清楚,但可能会影响疗效、不良事件和长期免疫能力。由于缺乏专门针对这些问题的临床研究,来自临床实践的观察结果对于指导当前的管理算法具有特别重要的价值。在 Ferraro 等人在该杂志上发表的一项研究的推动下,我们着手提供关于在活跃的 RMS 患者中从芬戈莫德转换为另一种 DMT 的有效性和安全性的已发表真实世界证据的概述。确定了 17 篇报告相关信息的出版物。文献表明,与从其他治疗药物转换的患者相比,从芬戈莫德转换的患者接受阿仑单抗或奥瑞珠单抗诱导的免疫细胞耗竭与复发风险增加和残疾恶化相关。然而,对于那他珠单抗和克拉屈滨的证据尚无定论。虽然缩短冲洗期可能会限制停用芬戈莫德后早期疾病复发,但没有强有力的证据表明冲洗期的持续时间或基线时的绝对淋巴细胞计数是预测长期疗效减弱的指标。需要进一步的真实世界研究来更好地了解临床试验中代表性不足的患者的结局。