Sundara Rajan Rajinikanth, Bhatia Anuj, Peng Philip W H, Gordon Allan S
Department of Anaesthesia and Pain Medicine, University of North Midlands NHS Trust, Staffordshire, United Kingdom.
Department of Anesthesia and Pain Management, University of Toronto, University Health Network-Toronto Western Hospital, Toronto, Ontario, Canada.
Can J Pain. 2017 Dec 15;1(1):216-225. doi: 10.1080/24740527.2017.1403846. eCollection 2017.
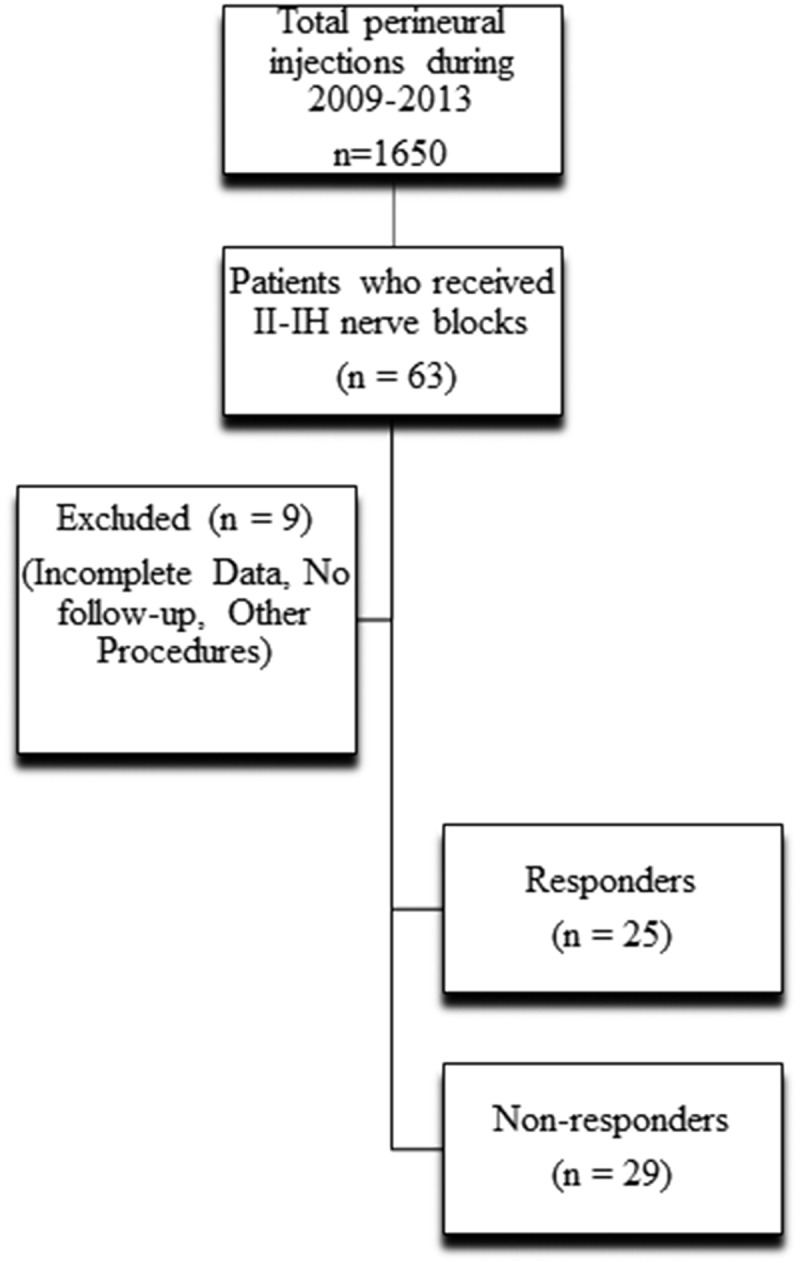
: Perineural local anaesthetic and steroid injections around ilioinguinal (II), iliohypogastric (IH), and genitofemoral (GF) nerves are often performed to treat chronic refractory neuropathic pain in the lower abdomen and groin, but there is a lack of published data on outcomes of these interventions. : The objective of this retrospective study was to evaluate analgesic outcomes of ultrasound-guided II, IH, and GF nerve blocks in patients with chronic neuropathic pain in the lower abdominal wall and groin. : Analgesic outcomes were assessed at 6 weeks after injections and patients were classified as "responders" if the numerical rating scale for pain score reduced by 30% or more. Variables analyzed for impact on outcomes included demographics, intensity of pain and duration, etiology, dose of opioid, presence of anxiety, depression, and diabetes mellitus. : In this cohort of 54 patients with severe baseline pain who had failed to receive analgesic benefit from recommended first- and second-line medications for neuropathic pain, 30 patients had history of surgery and 24 had pain secondary to visceral inflammatory pathologies. Twenty-five (46.3%) patients were identified as responders. A majority of the patients in this cohort had pain for more than one year. There was a higher incidence of diabetes mellitus in nonresponders compared to responders but the difference was not significant (14% and 0%, respectively; = 0.115). : Ultrasound-guided perineural steroids can ameliorate chronic refractory abdominal wall and groin neuropathic pain in patients who have failed to respond to conventional medical management at 6 weeks after the procedures.
在髂腹股沟神经(II)、髂腹下神经(IH)和生殖股神经(GF)周围进行神经周围局部麻醉和类固醇注射常用于治疗下腹部和腹股沟的慢性难治性神经性疼痛,但缺乏关于这些干预措施结果的已发表数据。本回顾性研究的目的是评估超声引导下对下腹壁和腹股沟慢性神经性疼痛患者进行II、IH和GF神经阻滞的镇痛效果。在注射后6周评估镇痛效果,如果疼痛评分数字评定量表降低30%或更多,则将患者分类为“反应者”。分析对结果有影响的变量包括人口统计学、疼痛强度和持续时间、病因、阿片类药物剂量、焦虑、抑郁和糖尿病的存在情况。在这组54例基线疼痛严重且未能从推荐的神经性疼痛一线和二线药物中获得镇痛益处的患者中,30例有手术史,24例疼痛继发于内脏炎症性病变。25例(46.3%)患者被确定为反应者。该队列中的大多数患者疼痛持续时间超过一年。无反应者的糖尿病发病率高于反应者,但差异不显著(分别为14%和0%;P = 0.115)。超声引导下神经周围注射类固醇可改善在术后6周对传统药物治疗无反应的患者的慢性难治性腹壁和腹股沟神经性疼痛。